Neville Iuri Santana, Ureña Francisco Matos, Quadros Danilo Gomes, Solla Davi J F, Lima Mariana Fontes, Simões Claudia Marquez, Vicentin Eduardo, Ribeiro Ulysses, Amorim Robson Luis Oliveira, Paiva Wellingson Silva, Teixeira Manoel Jacobsen
Instituto do Cancer do Estado de São Paulo do Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo, Av Dr Arnaldo 251 Cerqueira Cesar, CEP, São Paulo, 01246-000, Brazil.
Division of Neurosurgery, Hospital das Clinicas da Faculdade de Medicina da Universidade de São Paulo, Av Dr Arnaldo 251 Cerqueira Cesar, CEP, São Paulo, 01246-000, Brazil.
BMC Surg. 2020 May 14;20(1):105. doi: 10.1186/s12893-020-00767-y.
A daily algorithm for hospital discharge (DAHD) is a key point in the concept of Enhanced Recovery After Surgery (ERAS) protocol. We aimed to evaluate the length of stay (LOS), rate of complications, and hospital costs variances after the introduction of the DAHD compared to the traditional postoperative management of brain tumour patients.
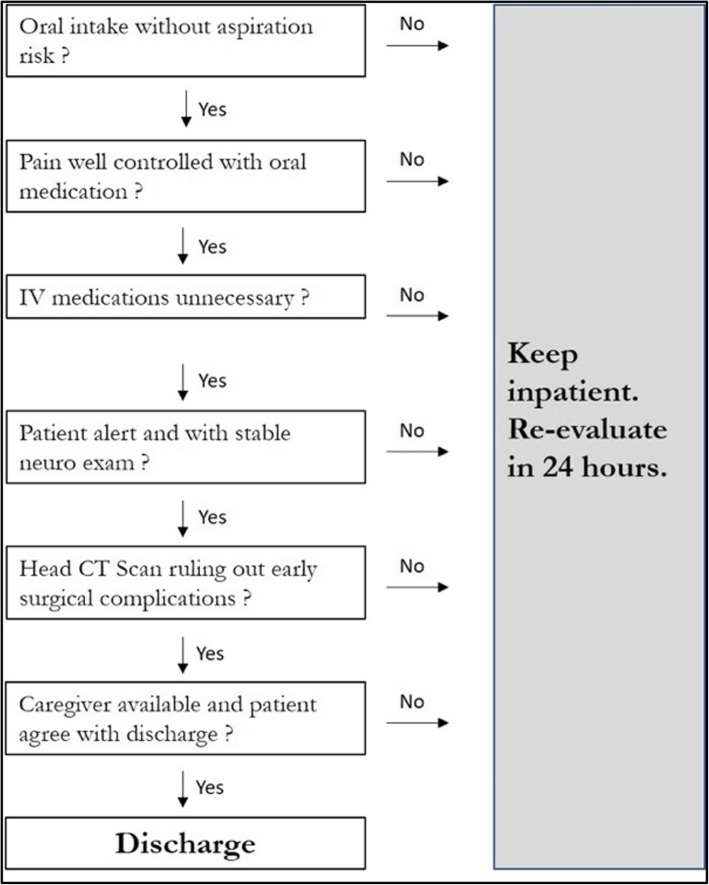
This is a cohort study with partial retrospective data collection. All consecutive patients who underwent brain tumour resection in 2017 were analysed. Demographics and procedure-related variables, as well as clinical outcomes, LOS and healthcare costs within 30 days after surgery were compared in patients before/pre-implementation and after/post-implementation the DAHD, which included: stable neurological examination; oral feeding without aspiration risk; pain control with oral medications; no intravenous medications. The algorithm was applied every morning and discharge was considered from day 1 after surgery if criteria was fulfilled. The primary outcome (LOS after surgery) analysis was adjusted for the preoperative performance status on a multivariable logistic regression model.
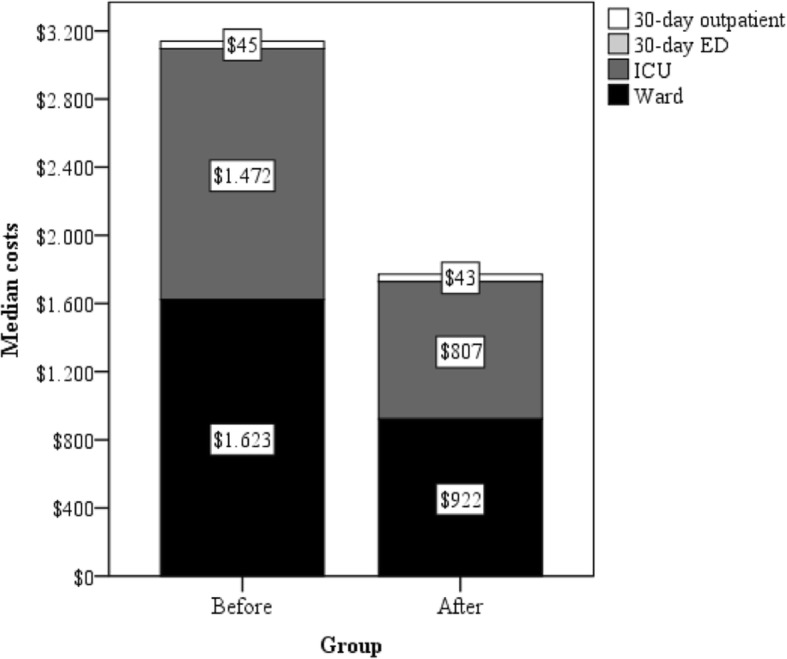
A total of 61 patients were studied (pre-implementation 32, post-implementation 29). The baseline demographic characteristics were similar between the groups. After the DAHD implementation, LOS decreased significantly (median 5 versus 3 days; p = 0.001) and the proportion of patients who were discharged on day 1 or 2 after surgery increased (44.8% vs 3.1%; p < 0.001). Major and minor complications rates, readmission rate, and unplanned return to hospital in 30-day follow-up were comparable between the groups. There was a significant reduction in the median costs of hospitalization in DAHD group (US$2135 vs US$2765, p = 0.043), mainly due to a reduction in median ward costs (US$922 vs US$1623, p = 0.009).
Early discharge after brain tumour surgery appears to be safe and inexpensive. The LOS and hospitalization costs were reduced without increasing readmission rate or postoperative complications.
每日出院算法(DAHD)是术后加速康复(ERAS)方案概念中的一个关键点。我们旨在评估与脑肿瘤患者传统术后管理相比,引入DAHD后的住院时间(LOS)、并发症发生率和医院成本差异。
这是一项采用部分回顾性数据收集的队列研究。分析了2017年所有连续接受脑肿瘤切除术的患者。比较了DAHD实施前/后患者的人口统计学和手术相关变量,以及术后30天内的临床结局、LOS和医疗费用,DAHD包括:神经系统检查稳定;无误吸风险的经口喂养;口服药物控制疼痛;无静脉用药。该算法每天早晨应用,如果符合标准,则从术后第1天开始考虑出院。在多变量逻辑回归模型中,对主要结局(术后LOS)分析进行了术前表现状态调整。
共研究了61例患者(实施前32例,实施后29例)。两组间基线人口统计学特征相似。实施DAHD后,LOS显著缩短(中位数5天对3天;p = 0.001),术后第1天或第2天出院的患者比例增加(44.8%对3.1%;p < 0.001)。两组间30天随访中的主要和次要并发症发生率、再入院率和非计划重返医院率相当。DAHD组住院费用中位数显著降低(2135美元对2765美元,p = 0.043),主要是由于病房费用中位数降低(922美元对1623美元,p = 0.009)。
脑肿瘤手术后早期出院似乎是安全且经济的。在不增加再入院率或术后并发症的情况下,LOS和住院费用降低。