Brenet Esteban, Barbe Coralie, Hoeffel Christine, Dubernard Xavier, Merol Jean-Claude, Fath Léa, Servagi-Vernat Stéphanie, Labrousse Marc
Department of Oto-Rhino-Laryngology, Head and Neck Surgery, Robert Debré University Hospital, 51100 Reims, France.
Clinical Research Unit, Robert Debré University Hospital, 51100 Reims, France.
Cancers (Basel). 2020 May 14;12(5):1234. doi: 10.3390/cancers12051234.
To investigate the predictive capacity of early post-treatment diffusion-weighted magnetic resonance imaging (MRI) for recurrence or tumor progression in patients with no tumor residue after chemo-radiotherapy (CRT) for head and neck squamous cell carcinoma, and, to assess the predictive capacity of pre-treatment diffusion-weighted MRI for persistent tumor residue post-CRT.
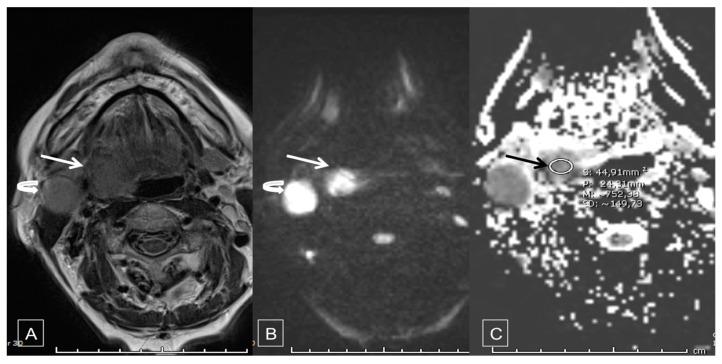
A single center cohort study was performed in one French hospital. All patients with squamous cell carcinoma receiving CRT (no surgical indication) were included. Two diffusion-weighted MRI were performed: one within 8 days before CRT and one 3 months after completing CRT with determination of median tumor apparent diffusion coefficient (ADC).
The primary endpoint was progression-free survival.
59 patients were included prior to CRT and 46 (78.0%) completed CRT. A post-CRT tumor residue was found in 19/46 (41.3%) patients. In univariate analysis, initial ADC was significantly lower in patients with residue post CRT (0.56 ± 0.11 versus 0.79 ± 0.13; < 0.001). When initial ADC was dichotomized at the median, initial ADC lower than 0.7 was significantly more frequent in patients with residue post CRT (73.7% versus 11.1%, < 0.0001). In multivariate analysis, only initial ADC lower than 0.7 was significantly associated with tumor residue (OR = 22.6; IC [4.9-103.6], < 0.0001). Among 26 patients without tumor residue after CRT and followed up until 12 months, 6 (23.1%) presented recurrence or progression. Only univariate analysis was performed due to a small number of events. The only factor significantly associated with disease progression or early recurrence was the delta ADC ( = 0.0009). When ADC variation was dichotomized at the median, patients with ADC variation greater than 0.7 had time of disease-free survival significantly longer than patients with ADC variation lower than 0.7 (377.5 [286-402] days versus 253 [198-370], < 0.0001). Conclusion and relevance: Diffusion-weighted MRI could be a technique that enables differentiation of patients with high potential for early recurrence for whom intensive post-CRT monitoring is mandatory. Prospective studies with more inclusions would be necessary to validate our results.
探讨头颈部鳞状细胞癌放化疗(CRT)后无肿瘤残留患者早期治疗后扩散加权磁共振成像(MRI)对复发或肿瘤进展的预测能力,并评估治疗前扩散加权MRI对CRT后持续性肿瘤残留的预测能力。
在一家法国医院进行了一项单中心队列研究。纳入所有接受CRT(无手术指征)的鳞状细胞癌患者。进行了两次扩散加权MRI检查:一次在CRT前8天内,另一次在完成CRT后3个月,测定肿瘤表观扩散系数(ADC)中位数。
主要终点是无进展生存期。
59例患者在CRT前纳入,46例(78.0%)完成了CRT。19/46例(41.3%)患者发现CRT后有肿瘤残留。单因素分析显示,CRT后有残留的患者初始ADC显著更低(0.56±0.11对0.79±0.13;<0.001)。当初始ADC以中位数进行二分法划分时,CRT后有残留的患者初始ADC低于0.7的情况显著更常见(73.7%对11.1%,<0.0001)。多因素分析显示,只有初始ADC低于0.7与肿瘤残留显著相关(OR=22.6;IC[4.9 - 103.6],<0.0001)。在26例CRT后无肿瘤残留且随访至12个月的患者中,6例(23.1%)出现复发或进展。由于事件数量少,仅进行了单因素分析。与疾病进展或早期复发显著相关的唯一因素是ADC变化量(=0.0009)。当ADC变化量以中位数进行二分法划分时,ADC变化量大于0.7的患者无病生存期显著长于ADC变化量低于0.7的患者(377.5[286 - 402]天对253[198 - 370]天,<0.0001)。结论与相关性:扩散加权MRI可能是一种能够区分早期复发高风险患者的技术,对于这些患者,CRT后强化监测是必要的。需要更多纳入病例的前瞻性研究来验证我们的结果。