Department of Vascular Medicine, Amsterdam Cardiovascular Science, Amsterdam, the Netherlands.
Department of Internal Medicine, Tergooi Hospitals, Hilversum, the Netherlands.
Br J Surg. 2020 Sep;107(10):1324-1333. doi: 10.1002/bjs.11665. Epub 2020 May 19.
In patients who undergo curative treatment for oesophageal cancer, risk estimates of venous thromboembolism (VTE), arterial thromboembolism and bleeding are needed to guide decisions about thromboprophylaxis.
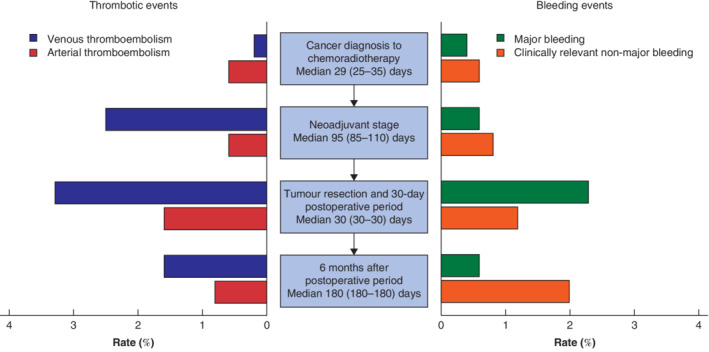
This was a single-centre, retrospective cohort study of patients with stage I-III oesophageal cancer who received neoadjuvant chemoradiation followed by oesophagectomy. The outcomes VTE, arterial thromboembolism, major bleeding, clinically relevant non-major bleeding and mortality were analysed for four consecutive cancer treatment stages (from diagnosis to neoadjuvant chemoradiotherapy, during neoadjuvant treatment, 30-day postoperative period, and up to 6 months after postoperative period).
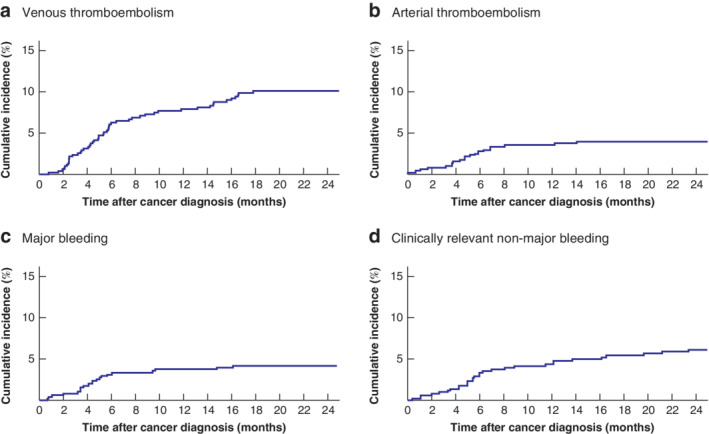
Some 511 patients were included. The 2-year survival rate was 67·3 (95 per cent c.i. 63·2 to 71·7) per cent. During the 2-year follow-up, 50 patients (9·8 per cent) developed VTE, 20 (3·9 per cent) arterial thromboembolism, 21 (4·1 per cent) major bleeding and 30 (5·9 per cent) clinically relevant non-major bleeding. The risk of these events was substantial at all treatment stages. Despite 30-day postoperative thromboprophylaxis, 17 patients (3·3 per cent) developed VTE after surgery. Patients with VTE had worse survival (time-varying hazard ratio 1·81, 95 per cent c.i. 1·25 to 2·64). Most bleeding events occurred around the time of medical intervention, and approximately one-half during concomitant use of prophylactic or therapeutic anticoagulation.
Patients with oesophageal cancer undergoing neoadjuvant chemoradiotherapy and surgery are at substantial risk of thromboembolic and bleeding events throughout all stages of treatment. Survival is worse in patients with thromboembolic events during follow-up.
在接受根治性治疗的食管癌患者中,需要评估静脉血栓栓塞症(VTE)、动脉血栓栓塞症和出血风险,以指导血栓预防决策。
这是一项单中心、回顾性队列研究,纳入了接受新辅助放化疗后行食管癌切除术的 I-III 期食管癌患者。分析了 4 个连续的癌症治疗阶段(从诊断到新辅助放化疗、新辅助治疗期间、术后 30 天和术后 6 个月)的 VTE、动脉血栓栓塞症、大出血、临床相关非大出血和死亡率等结局。
共纳入 511 例患者。2 年生存率为 67.3%(95%可信区间 63.2%至 71.7%)。在 2 年随访期间,50 例患者(9.8%)发生 VTE,20 例(3.9%)发生动脉血栓栓塞症,21 例(4.1%)发生大出血,30 例(5.9%)发生临床相关非大出血。在所有治疗阶段,这些事件的风险都很大。尽管术后 30 天进行了预防性抗凝治疗,但仍有 17 例(3.3%)患者发生术后 VTE。发生 VTE 的患者生存状况较差(时变风险比 1.81,95%可信区间 1.25 至 2.64)。大多数出血事件发生在医疗干预的时间附近,大约一半发生在预防性或治疗性抗凝药物同时使用时。
接受新辅助放化疗和手术治疗的食管癌患者在治疗的所有阶段都存在较大的血栓栓塞和出血风险。在随访期间发生血栓栓塞事件的患者生存状况更差。