Montreuil Julien, Saleh Joseph, Cresson Thierry, De Guise Jacques A, Lavoie Frédéric
Laboratoire de recherche en Imagerie et Orthopédie de l'ETS, Montréal, Québec, Canada.
McGill Division of Orthopaedic Surgery, Montréal General Hospital, Montréal, Québec, Canada.
Orthop J Sports Med. 2020 Apr 29;8(4):2325967120915709. doi: 10.1177/2325967120915709. eCollection 2020 Apr.
The femoral-sided anatomic footprint of the anterior cruciate ligament (ACL) has been widely studied during the past decades. Nonanatomic placement is an important cause of ACL reconstruction (ACLR) failure.
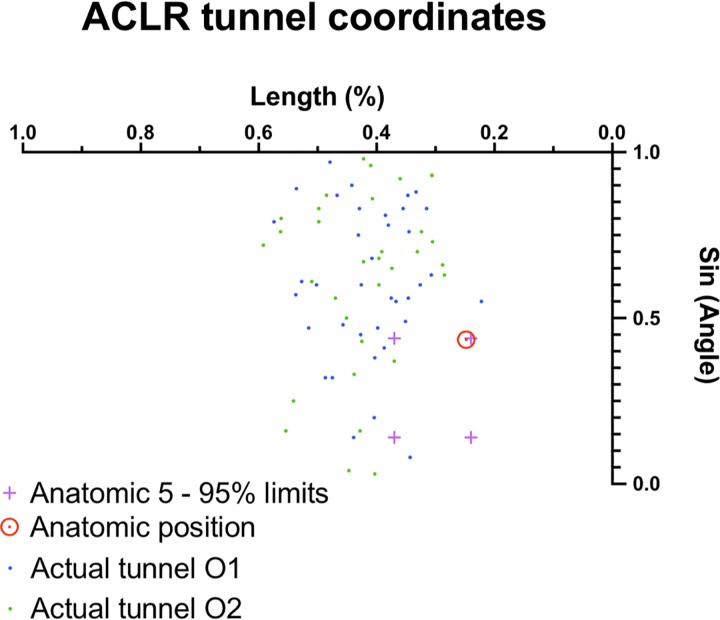
To describe femoral tunnel placement in ACLR through use of a comprehensive 3-dimensional (3D) cylindrical coordinate system combining both the traditional clockface technique and the quadrant method. Our objective was to validate this technique and evaluate its reproducibility.
Descriptive laboratory study.
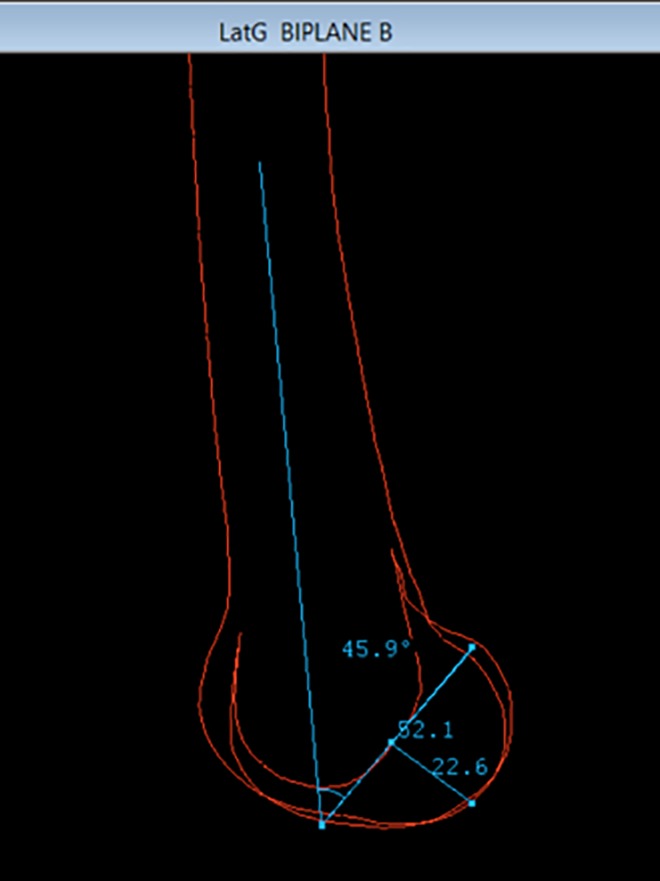
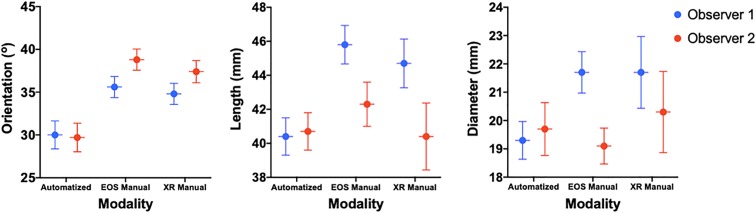
The EOS Imaging System was used to make 3D models of the knee for 37 patients who had undergone ACLR. We designed an automated cylindrical reference software program individualized to the distal femoral morphology of each patient. Cylinder parameters were collected from 2 observers' series of 3D models. Each independent observer also manually measured the corresponding parameters using a lateral view of the 3D contours and a 2-dimensional stereoradiographic image for the corresponding patient.
The average cylinder produced from the first observer's EOS 3D models had a 30.0° orientation (95% CI, 28.4°-31.5°), 40.4 mm length (95% CI, 39.3-41.4 mm), and 19.3 mm diameter (95% CI, 18.6-20.0 mm). For the second observer, these measurements were 29.7° (95% CI, 28.1°-31.3°), 40.7 mm (95% CI, 39.7-41.8 mm), and 19.7 mm (95% CI, 18.8-20.6 mm), respectively. Our method showed moderate intertest intraclass correlation among all 3 measuring techniques for both length ( = 0.68) and diameter ( = 0.63) but poor correlation for orientation ( = 0.44). In terms of interobserver reproducibility of the automated EOS 3D method, similar results were obtained: moderate to excellent correlations for length ( = 0.95; < .001) and diameter ( = 0.66; < .001) but poor correlation for orientation ( = 0.29; < .08). With this reference system, we were able to describe the placement of each individual femoral tunnel aperture, averaging a difference of less than 10 mm from the historical anatomic description by Bernard et al.
This novel 3D cylindrical coordinate system using biplanar, stereoradiographic, low-irradiation imaging showed a precision comparable with standard manual measurements for ACLR femoral tunnel placement. Our results also suggest that automated cylinders issued from EOS 3D models show adequate accuracy and reproducibility.
This technique will open multiple possibilities in ACLR femoral tunnel placement in terms of preoperative planning, postoperative feedback, and even intraoperative guidance with augmented reality.
在过去几十年中,前交叉韧带(ACL)股骨侧的解剖足迹已得到广泛研究。非解剖位置放置是ACL重建(ACLR)失败的一个重要原因。
通过使用结合传统钟面技术和象限法的综合三维(3D)圆柱坐标系来描述ACLR中股骨隧道的放置。我们的目标是验证该技术并评估其可重复性。
描述性实验室研究。
使用EOS成像系统为37例接受ACLR的患者制作膝关节的3D模型。我们设计了一个针对每位患者股骨远端形态个性化的自动圆柱参考软件程序。从2名观察者的3D模型系列中收集圆柱参数。每位独立观察者还使用3D轮廓的侧视图和相应患者的二维立体放射图像手动测量相应参数。
第一位观察者的EOS 3D模型生成的平均圆柱的方向为30.0°(95%CI,28.4° - 31.5°),长度为40. .4 mm(95%CI,39.3 - 41.4 mm),直径为19.3 mm(95%CI,18.6 - 20.0 mm)。对于第二位观察者,这些测量值分别为29.7°(95%CI,28.1° - 31.3°),40.7 mm(95%CI,39.7 - 41.8 mm)和19.7 mm(95%CI,18.8 - 20.6 mm)。我们的方法在长度( = 0.68)和直径( = 0.63)的所有3种测量技术之间显示出中等的组内相关,但在方向上相关性较差( = 0.44)。就自动EOS 3D方法的观察者间可重复性而言,获得了类似的结果:长度相关性中等至优秀( = 0.95; <.001),直径相关性中等( = 0.66; <.001),但方向相关性较差( = 0.29; <.08)。使用该参考系统,我们能够描述每个个体股骨隧道孔的位置,与Bernard等人的历史解剖描述平均相差不到10 mm。
这种使用双平面、立体放射、低辐射成像的新型3D圆柱坐标系在ACLR股骨隧道放置方面显示出与标准手动测量相当的精度。我们的结果还表明,从EOS 3D模型生成的自动圆柱显示出足够的准确性和可重复性。
该技术将在ACLR股骨隧道放置的术前规划、术后反馈甚至术中增强现实引导方面开辟多种可能性。