Percy military teaching hospital, Clamart, France; Val-de-Grâce military medical academy, Paris, France.
Percy military teaching hospital, Clamart, France.
Anaesth Crit Care Pain Med. 2020 Jun;39(3):333-339. doi: 10.1016/j.accpm.2020.05.008. Epub 2020 May 17.
Relying on capacity increases and patient transfers to deal with the huge and continuous inflow of COVID-19 critically ill patients is a strategy limited by finite human and logistical resources.
Prioritising both critical care initiation and continuation is paramount to save the greatest number of lives. It enables to allocate scarce resources in priority to those with the highest probability of benefiting from them. It is fully ethical provided it relies on objective and widely shared criteria, thus preventing arbitrary decisions and guaranteeing equity. Prioritisation seeks to fairly allocate treatments, maximise saved lives, gain indirect life benefits from prioritising exposed healthcare and similar workers, give priority to those most penalised as a last resort, and apply similar prioritisation schemes to all patients.
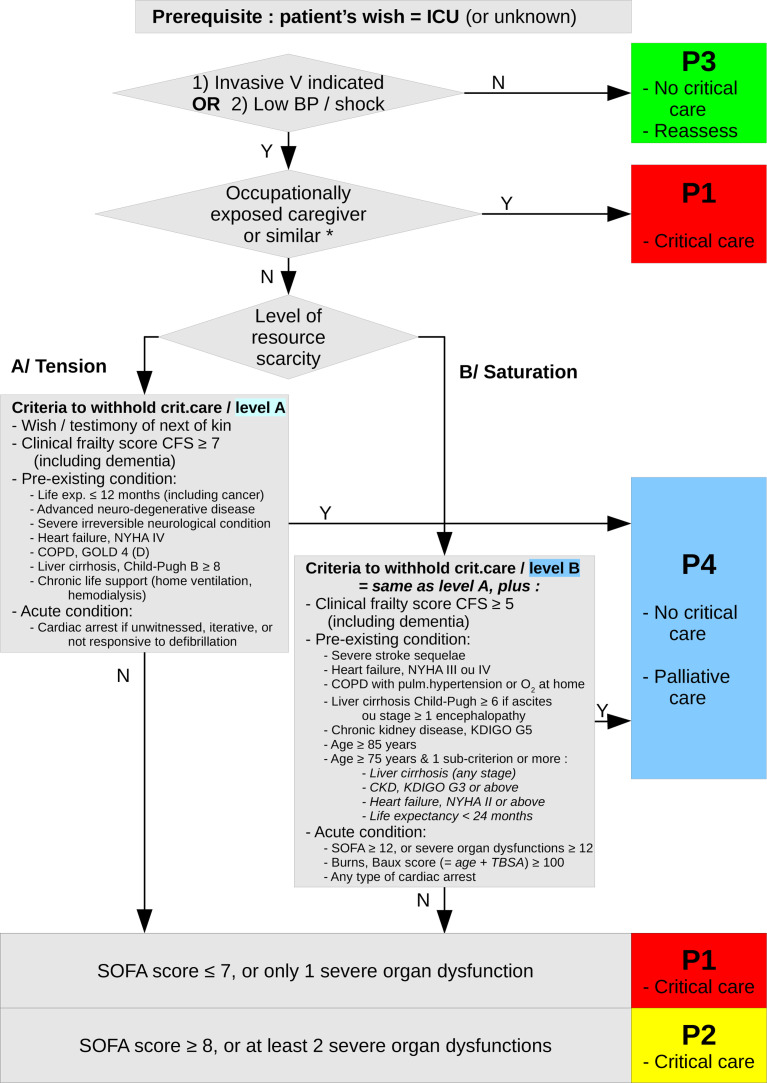
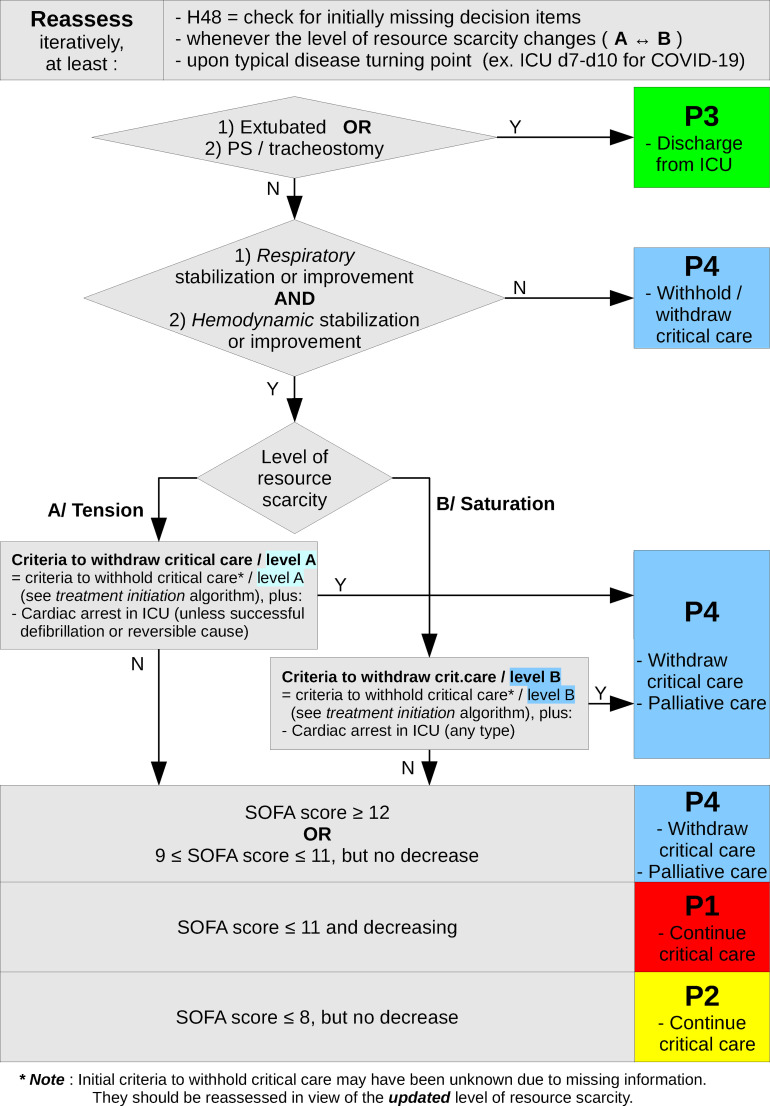
Prioritisation schemes and their criteria are adjusted to the level of resource scarcity: strain (level A) or saturation (level B). Prioritisation yields a four level priority for initiation or continuation of critical care: P1-high priority, P2-intermediate priority, P3-not needed, P4-not appropriate. Prioritisation schemes take into account the patient's wishes, clinical frailty, pre-existing chronic condition, along with severity and evolution of acute condition. Initial priority level must be reassessed, at least after 48h once missing decision elements are available, at the typical turning point in the disease's natural history (ICU days 7 to 10 for COVID-19), and each time resource scarcity levels change. For treatments to be withheld or withdrawn, a collegial decision-making process and information of patient and/or next of kin are paramount.
Prioritisation strategy is bound to evolve with new knowledge and with changes within the epidemiological situation.
依靠增加容量和转移患者来应对 COVID-19 重症患者的巨大且持续涌入,这种策略受到有限的人力和后勤资源的限制。
优先考虑重症监护的启动和持续,对于挽救尽可能多的生命至关重要。这使得能够优先将稀缺资源分配给最有可能从中受益的患者。只要它依赖于客观和广泛共享的标准,就完全符合道德规范,从而防止任意决策并保证公平。优先级排序旨在公平分配治疗方法,最大限度地挽救生命,从优先考虑暴露于医疗保健和类似工作的医护人员中获得间接生命获益,作为最后手段优先考虑那些受到最大惩罚的人,并对所有患者应用类似的优先级排序方案。
根据资源稀缺程度调整优先级排序方案及其标准:紧张(A 级)或饱和(B 级)。优先级排序为重症监护的启动或持续提供四个优先级:P1-高优先级,P2-中优先级,P3-不需要,P4-不合适。优先级排序方案考虑了患者的意愿、临床脆弱性、预先存在的慢性疾病,以及急性疾病的严重程度和演变。必须在至少 48 小时后,一旦获得缺失的决策要素,在疾病自然史的典型转折点(COVID-19 的 ICU 天数 7 至 10 天),以及每次资源稀缺水平发生变化时,重新评估初始优先级级别。对于需要暂停或撤回的治疗,需要进行同行评议决策过程,并告知患者和/或家属。
优先级排序策略必然会随着新知识和流行病学情况的变化而发展。