University of Toronto, Toronto, Ontario, Canada.
ICES, Toronto, Ontario, Canada.
PLoS Med. 2020 May 19;17(5):e1003104. doi: 10.1371/journal.pmed.1003104. eCollection 2020 May.
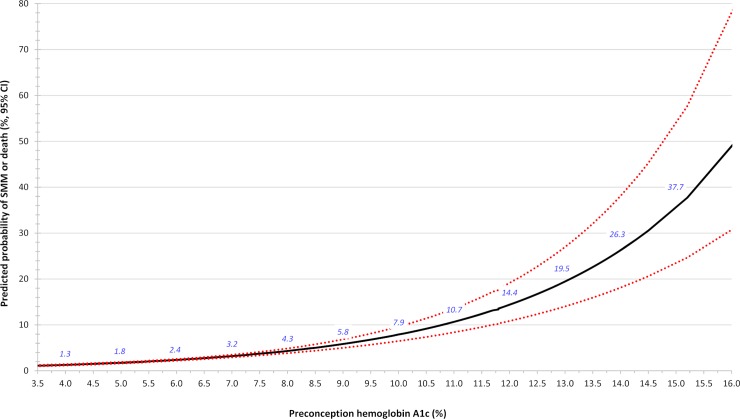
The relation between prepregnancy average glucose concentration and a woman's risk of severe maternal morbidity (SMM) is unknown. The current study evaluated whether an elevated preconception hemoglobin A1c (A1c) is associated with SMM or maternal death among women with and without known prepregnancy diabetes mellitus (DM).
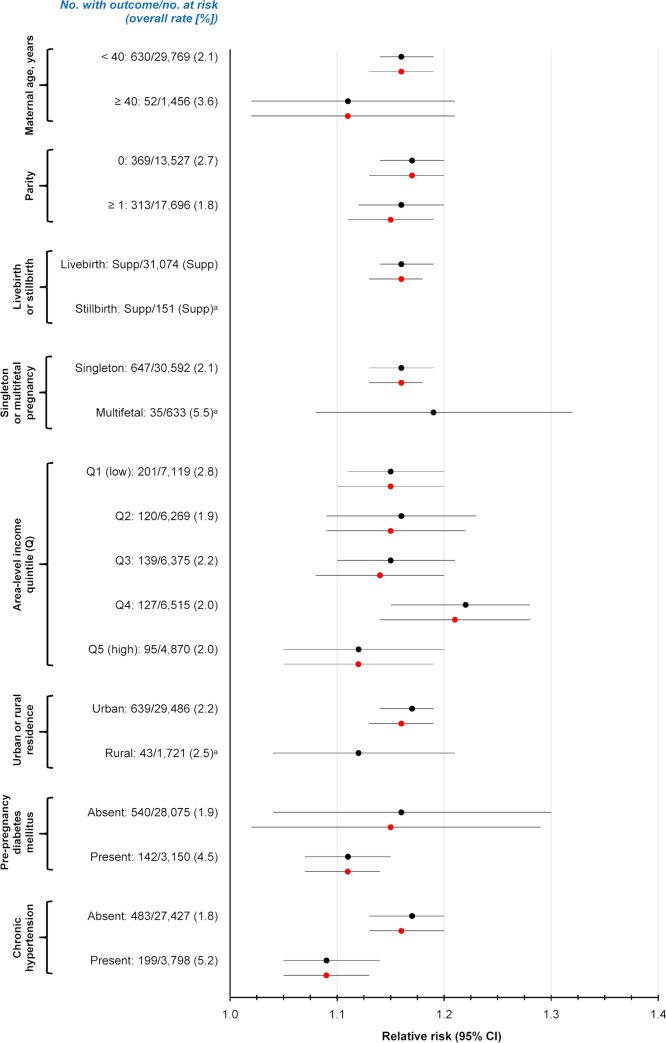
A population-based cohort study was completed in Ontario, Canada, where there is universal healthcare. The main cohort included 31,225 women aged 16-50 years with a hospital live birth or stillbirth from 2007 to 2015, and who had an A1c measured within 90 days before conception, including 28,075 women (90%) without known prepregnancy DM. The main outcome was SMM or maternal mortality from 23 weeks' gestation up to 42 days postpartum. Relative risks (RRs) were generated using modified Poisson regression, adjusting for the main covariates of maternal age, multifetal pregnancy, world region of origin, and tobacco/drug dependence. The mean maternal age was 31.1 years. Overall, SMM or death arose among 682 births (2.2%). The RR of SMM or death was 1.16 (95% CI 1.14-1.19; p < 0.001) per 0.5% increase in A1c and 1.16 (95% CI 1.13-1.18; p < 0.001) after adjusting for the main covariates. The adjusted relative risk (aRR) was increased among those with (1.11, 95% CI 1.07-1.14; p < 0.001) and without (1.15, 95% CI 1.02-1.29; p < 0.001) known prepregnancy diabetes, and upon further adjusting for body mass index (BMI) (1.15, 95% CI 1.11-1.20; p < 0.001), or chronic hypertension and prepregnancy serum creatinine (1.11, 95% CI 1.04-1.18; p = 0.002). The aRR of SMM or death was 1.31 (95% CI 1.06-1.62; p = 0.01) in those with a preconception A1c of 5.8%-6.4%, and 2.84 (95% CI 2.31-3.49; p < 0.001) at an A1c > 6.4%, each relative to an A1c < 5.8%. Among those without previously recognized prepregnancy diabetes and whose A1c was >6.4%, the aRR of SMM or death was 3.25 (95% CI 1.76-6.00; p < 0.001). Study limitations include that selection bias may have incorporated less healthy women tested for A1c, and BMI was unknown for many women.
Our findings indicate that women with an elevated A1c preconception may be at higher risk of SMM or death in pregnancy or postpartum, including those without known prepregnancy DM.
目前尚不清楚孕妇平均血糖浓度与严重产妇发病率(SMM)之间的关系。本研究评估了在患有和不患有已知孕前糖尿病(DM)的女性中,孕前血红蛋白 A1c(A1c)升高是否与 SMM 或产妇死亡相关。
在加拿大安大略省进行了一项基于人群的队列研究,该省提供全民医疗保健。主要队列包括 2007 年至 2015 年期间在医院分娩或死产的 31225 名 16-50 岁的女性,她们在受孕前 90 天内测量了 A1c,其中包括 28075 名(90%)无已知孕前 DM 的女性。主要结局是从妊娠 23 周起至产后 42 天的 SMM 或产妇死亡。使用修正泊松回归生成相对风险(RR),并调整了产妇年龄、多胎妊娠、原籍世界区域和烟草/药物依赖等主要协变量。平均产妇年龄为 31.1 岁。总体而言,有 682 例分娩(2.2%)发生了 SMM 或死亡。A1c 每增加 0.5%,SMM 或死亡的 RR 为 1.16(95%CI 1.14-1.19;p<0.001),调整主要协变量后为 1.16(95%CI 1.13-1.18;p<0.001)。在有(1.11,95%CI 1.07-1.14;p<0.001)和无(1.15,95%CI 1.02-1.29;p<0.001)已知孕前糖尿病的患者中,调整后的相对风险(aRR)增加,进一步调整体重指数(BMI)后(1.15,95%CI 1.11-1.20;p<0.001),或慢性高血压和孕前血清肌酐(1.11,95%CI 1.04-1.18;p=0.002)。A1c 为 5.8%-6.4%的患者 SMM 或死亡的 aRR 为 1.31(95%CI 1.06-1.62;p=0.01),A1c>6.4%的患者 SMM 或死亡的 aRR 为 2.84(95%CI 2.31-3.49;p<0.001),与 A1c<5.8%相比。在那些没有先前确诊的孕前糖尿病且 A1c>6.4%的患者中,SMM 或死亡的 aRR 为 3.25(95%CI 1.76-6.00;p<0.001)。研究的局限性包括选择偏差可能包括接受 A1c 检测的身体状况较差的女性,并且许多女性的 BMI 未知。
我们的研究结果表明,孕前 A1c 升高的女性在怀孕期间或产后发生 SMM 或死亡的风险可能更高,包括那些没有已知孕前 DM 的女性。