Shimizu Takuto, Miyake Makito, Hori Shunta, Ichikawa Kazuki, Omori Chihiro, Iemura Yusuke, Owari Takuya, Itami Yoshitaka, Nakai Yasushi, Anai Satoshi, Tomioka Atsushi, Tanaka Nobumichi, Fujimoto Kiyohide
Department of Urology, Nara Medical University, 840 Shijo-cho, Kashihara, Nara 634-8522, Japan.
Department of Urology, Saiseikai Chuwa Hospital, 323 Ooazaabe, Sakurai, Nara 633-0054, Japan.
Diagnostics (Basel). 2020 May 15;10(5):310. doi: 10.3390/diagnostics10050310.
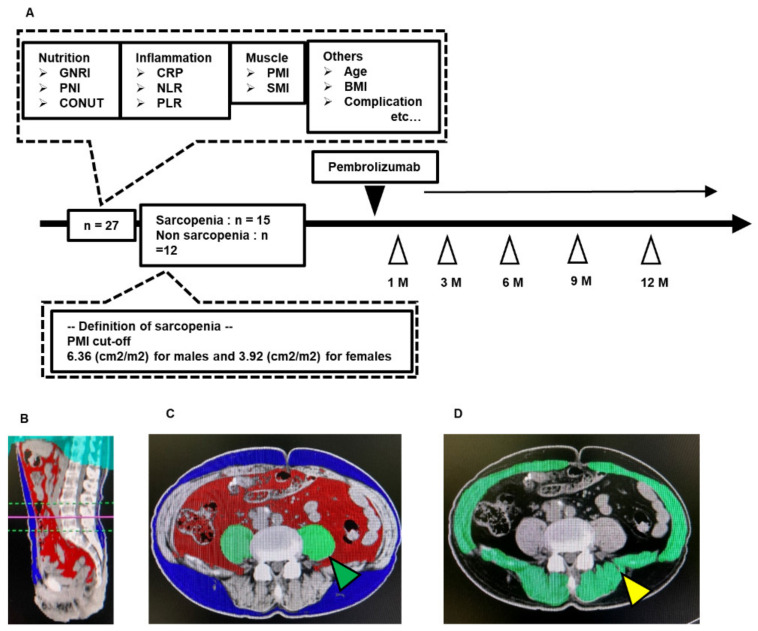
Sarcopenia is a muscle loss syndrome known as a risk factor of various carcinomas. The impact of sarcopenia and sarcopenia-related inflammatory/nutritional markers in metastatic urothelial carcinoma (mUC) treated with pembrolizumab was unknown, so this retrospective study of 27 patients was performed. Psoas muscle mass index (PMI) was calculated by bilateral psoas major muscle area at the L3 with computed tomography. The cut-off PMI value for sarcopenia was defined as ≤6.36 cm/m for men and ≤3.92 cm/m for women. Neutrophil-to-lymphocyte ratio (NLR) ≥ 4.0 and sarcopenia correlated with significantly shorter progression-free survival (PFS) (hazard ratio (HR) 3.81, = 0.020; and HR 2.99, = 0.027, respectively). Multivariate analyses identified NLR ≥ 4.0 and sarcopenia as independent predictors for PFS (HR 2.89, = 0.025; and HR 2.79, = 0.030, respectively). Prognostic nutrition index < 45, NLR ≥ 4.0 and sarcopenia were correlated with significantly worse for overall survival (OS) (HR 3.44, = 0.046; HR 4.26, = 0.024; and HR 3.92, = 0.012, respectively). Multivariate analyses identified sarcopenia as an independent predictor for OS (HR 4.00, = 0.026). Furthermore, a decrease in PMI ≥ 5% in a month was an independent predictor of PFS and OS (HR 12.8, = 0.008; and HR 6.21, = 0.036, respectively). Evaluation of sarcopenia and inflammatory/nutritional markers may help in the management of mUC with pembrolizumab.
肌肉减少症是一种肌肉流失综合征,已知是多种癌症的危险因素。肌肉减少症及与肌肉减少症相关的炎症/营养标志物对接受帕博利珠单抗治疗的转移性尿路上皮癌(mUC)的影响尚不清楚,因此对27例患者进行了这项回顾性研究。通过计算机断层扫描测量L3水平双侧腰大肌面积来计算腰大肌质量指数(PMI)。肌肉减少症的PMI临界值定义为男性≤6.36 cm/m,女性≤3.92 cm/m。中性粒细胞与淋巴细胞比值(NLR)≥4.0和肌肉减少症与无进展生存期(PFS)显著缩短相关(风险比[HR]分别为3.81,P = 0.020;以及HR 2.99,P = 0.027)。多变量分析确定NLR≥4.0和肌肉减少症是PFS的独立预测因素(HR分别为2.89,P = 0.025;以及HR 2.79,P = 0.030)。预后营养指数<45、NLR≥4.0和肌肉减少症与总生存期(OS)显著较差相关(HR分别为3.44,P = 0.046;HR 4.26,P = 0.024;以及HR 3.92,P = 0.012)。多变量分析确定肌肉减少症是OS的独立预测因素(HR 4.00,P = 0.026)。此外,一个月内PMI下降≥5%是PFS和OS的独立预测因素(HR分别为12.8,P = 0.008;以及HR 6.21,P = 0.036)。评估肌肉减少症和炎症/营养标志物可能有助于帕博利珠单抗治疗mUC的管理。