Jakubowski Jonathan K, Patel Rosemina, Buddharaju Venkata
Internal Medicine, Chicago Medical School - Rosalind Franklin University of Medicine and Science, North Chicago, USA.
Nephrology, Chicago Medical School - Rosalind Franklin University of Medicine and Science, North Chicago, USA.
Cureus. 2020 May 14;12(5):e8125. doi: 10.7759/cureus.8125.
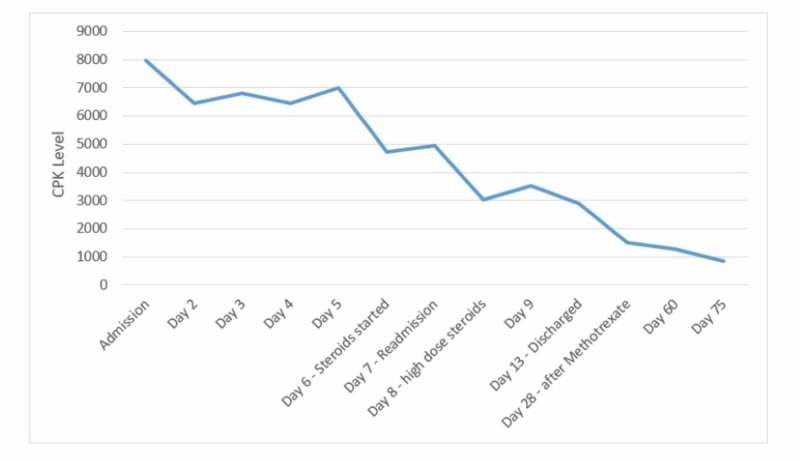
Rhabdomyolysis is a clinical syndrome with a wide range of presentations; it results in muscle necrosis and release of intracellular muscle contents into the circulation. Inflammatory myopathies are a rare cause of rhabdomyolysis. We present a case of a 46-year-old male with a two-week history of progressively worsening diffuse muscle pain after he had been prescribed omeprazole one month prior. A creatine phosphokinase (CPK) elevation was noted, which persisted despite treatment with IV fluids, sodium bicarbonate, and close correction of electrolytes. Further workup, including autoimmune and infectious etiologies, was notable for elevated antinuclear antibodies (ANA), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Furthermore, a muscle biopsy showed evidence of endomysial inflammatory cells, consistent with a diagnosis of polymyositis. Steroids were initiated with significant improvement in symptoms and a decrease in CPK levels. The patient was discharged on a tapering dose of steroids and, on follow-up with the rheumatologist, transitioned to methotrexate with control of symptoms. In patients with rhabdomyolysis who do not respond to first-line therapy, obtaining a detailed medication history and screening with ANA and ESR are encouraged. Given the link between medication and autoimmune disease, clinicians should consider autoimmune myopathy in the differential for cases with persistently elevated creatine kinase. Prompt diagnosis with early initiation of immunosuppressive medication may improve outcomes and avoid complications associated with untreated rhabdomyolysis or polymyositis.
横纹肌溶解症是一种临床表现多样的临床综合征;它会导致肌肉坏死,并使细胞内的肌肉成分释放到循环系统中。炎性肌病是横纹肌溶解症的罕见病因。我们报告一例46岁男性病例,该患者在一个月前服用奥美拉唑后,出现了为期两周的进行性加重的弥漫性肌肉疼痛。发现其肌酸磷酸激酶(CPK)升高,尽管给予静脉输液、碳酸氢钠治疗以及密切纠正电解质,该指标仍持续升高。进一步检查,包括自身免疫和感染性病因检查,结果显示抗核抗体(ANA)、红细胞沉降率(ESR)和C反应蛋白(CRP)升高。此外,肌肉活检显示存在肌内膜炎性细胞,符合多发性肌炎的诊断。开始使用类固醇治疗后,症状有显著改善,CPK水平下降。患者出院时服用逐渐减量的类固醇,在风湿科医生的随访中,转为使用甲氨蝶呤,症状得到控制。对于对一线治疗无反应的横纹肌溶解症患者,建议获取详细的用药史,并进行ANA和ESR筛查。鉴于药物与自身免疫性疾病之间的联系,临床医生在鉴别肌酸激酶持续升高的病例时应考虑自身免疫性肌病。早期启动免疫抑制药物进行快速诊断可能会改善预后,并避免与未治疗的横纹肌溶解症或多发性肌炎相关的并发症。