Douros Konstantinos, Everard Mark L
Third Department of Paediatrics, Attikon Hospital, University of Athens School of Medicine, Athens, Greece.
Division of Paediatrics and Child Health, Perth Children's Hospital, University of Western Australia, Nedlands, WA, Australia.
Front Pediatr. 2020 May 5;8:218. doi: 10.3389/fped.2020.00218. eCollection 2020.
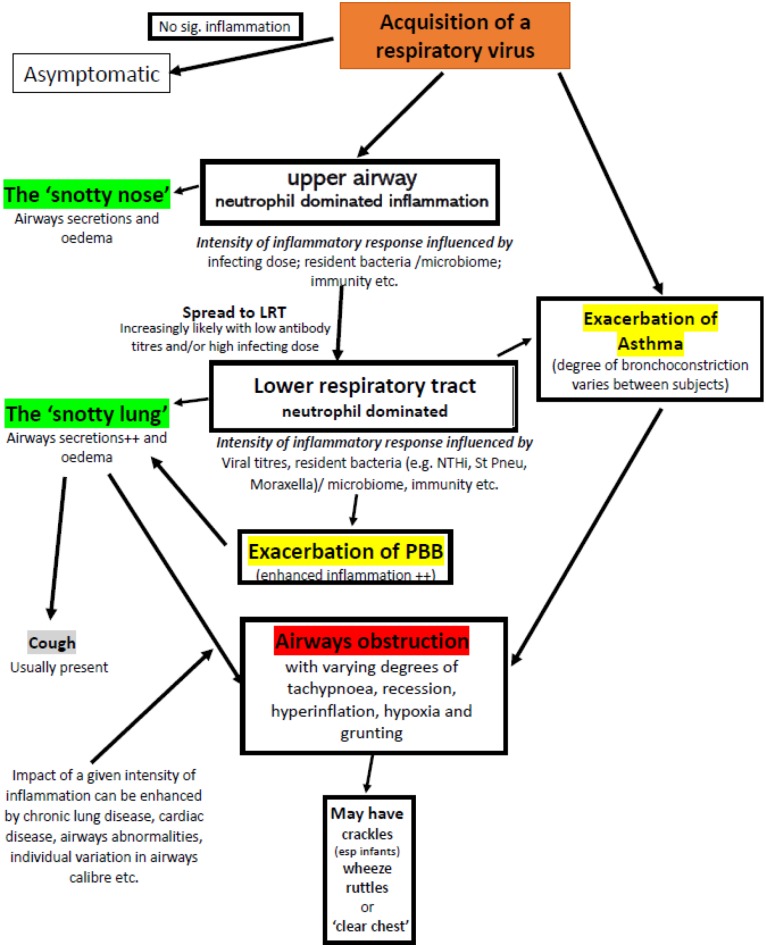
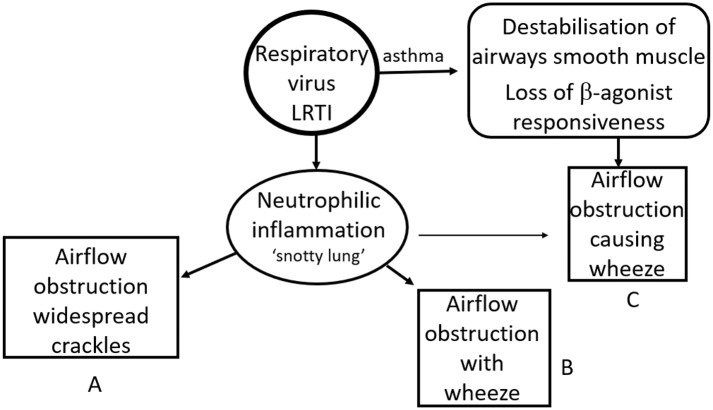
The diagnosis and management of infants and children with a significant viral lower respiratory tract illness remains the subject of much debate and little progress. Over the decades various terms for such illnesses have been in and fallen out of fashion or have evolved to mean different things to different clinicians. Terms such as "bronchiolitis," "reactive airways disease," "viral wheeze," and many more are used to describe the same condition and the same term is frequently used to describe illnesses caused by completely different dominant pathologies. This lack of clarity is due, in large part, to a failure to understand the basic underlying inflammatory and associated processes and, in part, due to the lack of a simple test to identify a condition such as asthma. Moreover, there is a lack of insight into the fact that the same pathology can produce different clinical signs at different ages. The consequence is that terminology and fashions in treatment have tended to go around in circles. As was noted almost 60 years ago, amongst pre-school children with a viral LRTI and airways obstruction there are those with a "viral bronchitis" and those with asthma. In the former group, a neutrophil dominated inflammation response is responsible for the airways' obstruction whilst amongst asthmatics much of the obstruction is attributable to bronchoconstriction. The airways obstruction in the former group is predominantly caused by airways secretions and to some extent mucosal oedema (a "snotty lung"). These patients benefit from good supportive care including supplemental oxygen if required (though those with a pre-existing bacterial bronchitis will also benefit from antibiotics). For those with a viral exacerbation of asthma, characterized by bronchoconstriction combined with impaired b-agonist responsiveness, standard management of an exacerbation of asthma (including the use of steroids to re-establish bronchodilator responsiveness) represents optimal treatment. The difficulty is identifying which group a particular patient falls into. A proposed simplified approach to the nomenclature used to categorize virus associated LRTIs is presented based on an understanding of the underlying pathological processes and how these contribute to the physical signs.
患有严重病毒性下呼吸道疾病的婴幼儿的诊断和管理仍然是一个备受争议且进展甚微的话题。几十年来,用于描述此类疾病的各种术语流行一时又逐渐过时,或者演变成对不同临床医生有不同含义的词汇。诸如“细支气管炎”“反应性气道疾病”“病毒性喘息”等术语被用来描述同一种病症,而且同一个术语常常被用来描述由完全不同的主要病理引起的疾病。这种缺乏清晰度的情况,在很大程度上是由于未能理解基本的潜在炎症及相关过程,部分原因是缺乏一种简单的测试来识别诸如哮喘之类的病症。此外,人们没有认识到相同的病理在不同年龄会产生不同的临床体征。结果是,术语和治疗方式往往循环往复。正如近60年前所指出的,在患有病毒性下呼吸道感染和气道阻塞的学龄前儿童中,有患“病毒性支气管炎”的,也有患哮喘的。在前一组中,以中性粒细胞为主的炎症反应导致气道阻塞,而在哮喘患者中,大部分阻塞归因于支气管收缩。前一组中的气道阻塞主要由气道分泌物以及在某种程度上由黏膜水肿(“鼻涕肺”)引起。这些患者受益于良好的支持性护理,如有需要可补充氧气(不过患有既往细菌性支气管炎的患者也会受益于抗生素)。对于那些以支气管收缩合并β受体激动剂反应性受损为特征的哮喘病毒加重患者,哮喘加重的标准管理(包括使用类固醇来恢复支气管扩张剂反应性)是最佳治疗方法。困难在于确定某个特定患者属于哪一组。基于对潜在病理过程及其如何导致体征的理解,提出了一种用于对病毒相关下呼吸道感染进行分类的简化命名方法。