Department of Critical Care Services, Neuroscience Institute, Maine Medical Center, 22 Bramhall Street, Portland, ME, 04102, USA.
Department of Pharmacy, Mayo Clinic, 200 First Street SW, Rochester, MN, 55905, USA.
Neurocrit Care. 2021 Feb;34(1):102-111. doi: 10.1007/s12028-020-00986-4.
BACKGROUND/OBJECTIVE: Neurostimulants may improve or accelerate cognitive and functional recovery after intracerebral hemorrhage (ICH), ischemic stroke (IS), or subarachnoid hemorrhage (SAH), but few studies have described their safety and effectiveness in the intensive care unit (ICU). The objective of this study was to describe amantadine and modafinil administration practices during acute stroke care starting in the ICU and to evaluate safety and effectiveness.
Consecutive adult ICU patients treated with amantadine and/or modafinil following acute non-traumatic IS, ICH, or SAH were evaluated. Neurostimulant administration data were extracted from the electronic medication administration record, including medication (amantadine, modafinil, or both), starting dose, time from stroke to initiation, and whether the neurostimulant was continued at hospital discharge. Patients were considered responders if they met two of three criteria within 9 days of neurostimulant initiation: increase in Glasgow coma scale (GCS) score ≥ 3 points from pre-treatment baseline, improved wakefulness or participation documented in caregiver notes, or clinical improvement documented in physical or occupational therapy notes. Potential confounders of the effectiveness assessment and adverse drug effects were also recorded.
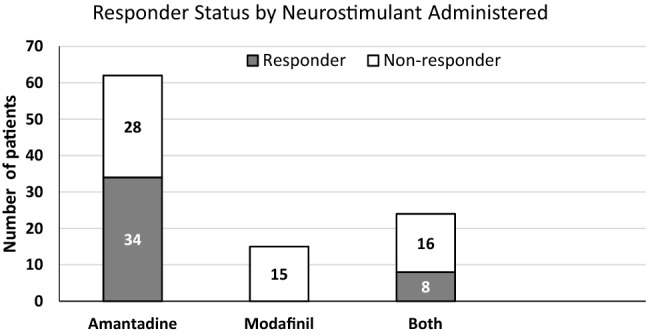
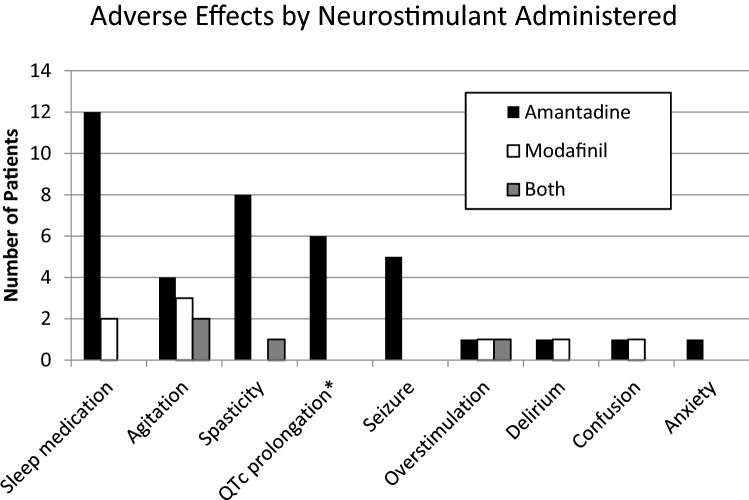
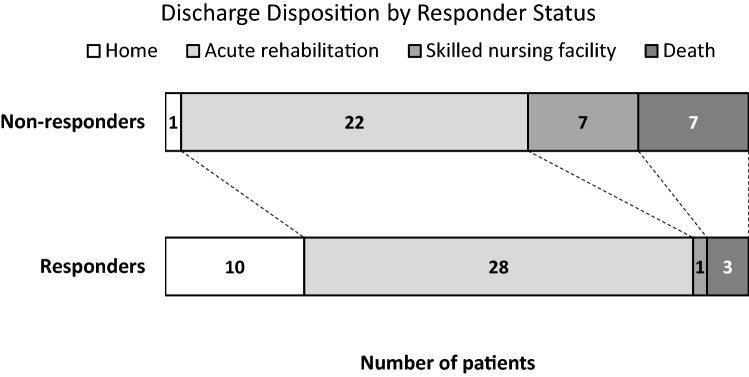
A total of 87 patients were evaluable during the 3.7-year study period, including 41 (47%) with ICH, 29 (33%) with IS, and 17 (20%) with SAH. The initial neurostimulant administered was amantadine in 71 (82%) patients, modafinil in 13 (15%), or both in 3 (3%) patients. Neurostimulants were initiated a median of 7 (4.25, 12.75) days post-stroke (range 1-27 days) for somnolence (77%), not following commands (32%), lack of eye opening (28%), or low GCS (17%). The most common starting dose was 100 mg twice daily for both amantadine (86%) and modafinil (54%). Of the 79 patients included in the effectiveness evaluation, 42 (53%) were considered responders, including 34/62 (55%) receiving amantadine monotherapy and 8/24 (33%) receiving both amantadine and modafinil at the time they met the definition of a responder. No patient receiving modafinil monotherapy was considered a responder. The median time from initiation to response was 3 (2, 5) days. Responders were more frequently discharged home or to acute rehabilitation compared to non-responders (90% vs 62%, p = 0.006). Among survivors, 63/72 (88%) were prescribed a neurostimulant at hospital discharge. The most common potential adverse drug effect was sleep disruption (16%).
Neurostimulant administration during acute stroke care may improve wakefulness. Future controlled studies with a neurostimulant administration protocol, prospective evaluation, and discretely defined response and safety criteria are needed to confirm these encouraging findings.
背景/目的:神经刺激剂可能改善或加速脑出血(ICH)、缺血性中风(IS)或蛛网膜下腔出血(SAH)后的认知和功能恢复,但很少有研究描述过它们在重症监护病房(ICU)中的安全性和有效性。本研究的目的是描述 ICU 中急性中风治疗开始时使用金刚烷胺和/或莫达非尼的情况,并评估其安全性和有效性。
连续评估了接受急性非创伤性 IS、ICH 或 SAH 后接受金刚烷胺和/或莫达非尼治疗的成年 ICU 患者。从电子药物管理记录中提取神经刺激剂给药数据,包括药物(金刚烷胺、莫达非尼或两者)、起始剂量、从中风到开始给药的时间以及出院时是否继续使用神经刺激剂。如果患者在神经刺激剂开始后 9 天内符合以下三个标准中的两个,即被认为是有反应者:GCS 评分较基线增加≥3 分、照护者记录的觉醒或参与度改善,或物理或职业治疗记录的临床改善。还记录了对有效性评估和药物不良反应的潜在混杂因素。
在 3.7 年的研究期间,共有 87 例患者可进行评估,其中 41 例(47%)为 ICH,29 例(33%)为 IS,17 例(20%)为 SAH。初始神经刺激剂为金刚烷胺的患者 71 例(82%),莫达非尼 13 例(15%),两者均用的 3 例(3%)。神经刺激剂的起始时间中位数为中风后 7(4.25,12.75)天(范围 1-27 天),用于治疗昏睡(77%)、不遵医嘱(32%)、无睁眼(28%)或 GCS 低(17%)。最常见的起始剂量为金刚烷胺 100mg,每日两次(86%),莫达非尼 50mg,每日两次(54%)。在 79 例接受有效性评估的患者中,42 例(53%)被认为是有反应者,包括接受金刚烷胺单药治疗的 34/62 例(55%)和接受金刚烷胺和莫达非尼联合治疗的 8/24 例(33%)。没有接受莫达非尼单药治疗的患者被认为是有反应者。从开始到反应的中位时间为 3(2,5)天。与无反应者相比,有反应者更常出院回家或到急性康复病房(90% vs 62%,p=0.006)。在幸存者中,63/72 例(88%)在出院时被处方了神经刺激剂。最常见的潜在药物不良反应是睡眠障碍(16%)。
急性中风治疗期间使用神经刺激剂可能会改善觉醒状态。需要进一步进行有神经刺激剂给药方案、前瞻性评估和明确界定的反应和安全性标准的对照研究,以证实这些令人鼓舞的发现。