Gastroenterology and Hepatology, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands
Gastroenterology and Hepatology, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Gut. 2021 Jan;70(1):30-39. doi: 10.1136/gutjnl-2020-320772. Epub 2020 May 21.
After treatment, achalasia patients often develop reflux symptoms. Aim of this case-control study was to investigate mechanisms underlying reflux symptoms in treated achalasia patients by analysing oesophageal function, acidification patterns and symptom perception.
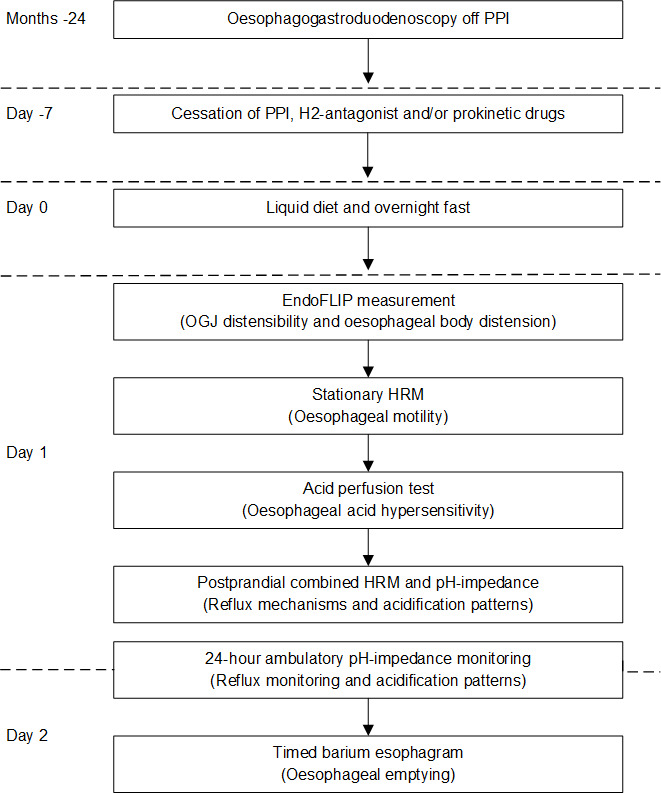
Forty treated achalasia patients (mean age 52.9 years; 27 (68%) men) were included, 20 patients with reflux symptoms (RS+; Gastro-Oesophageal Reflux Disease Questionnaire (GORDQ) ≥8) and 20 without reflux symptoms (RS-: GORDQ <8). Patients underwent measurements of oesophagogastric junction distensibility, high-resolution manometry, timed barium oesophagogram, 24 hours pH-impedance monitoring off acid-suppression and oesophageal perception for acid perfusion and distension. Presence of oesophagitis was assessed endoscopically.
Total acid exposure time during 24 hours pH-impedance was not significantly different between patients with (RS+) and without (RS-) reflux symptoms. In RS+ patients, acid fermentation was higher than in RS- patients (RS+: mean 6.6% (95% CI 2.96% to 10.2%) vs RS-: 1.8% (95% CI -0.45% to 4.1%, p=0.03) as well as acid reflux with delayed clearance (RS+: 6% (95% CI 0.94% to 11%) vs RS-: 3.4% (95% CI -0.34% to 7.18%), p=0.051). Reflux symptoms were not related to acid in both groups, reflected by a low Symptom Index. RS+ patients were highly hypersensitive to acid, with a much shorter time to heartburn perception (RS+: 4 (2-6) vs RS-:30 (14-30) min, p<0.001) and a much higher symptom intensity (RS+: 7 (4.8-9) vs RS-: 0.5 (0-4.5) Visual Analogue Scale, p<0.001) during acid perfusion. They also had a lower threshold for mechanical stimulation.
Reflux symptoms in treated achalasia are rarely caused by gastro-oesophageal reflux and most instances of oesophageal acidification are not reflux related. Instead, achalasia patients with post-treatment reflux symptoms demonstrate oesophageal hypersensitivity to chemical and mechanical stimuli, which may determine symptom generation.
贲门失弛缓症患者经治疗后常出现反流症状。本病例对照研究旨在通过分析食管功能、酸化模式和症状感知,探讨治疗后贲门失弛缓症患者发生反流症状的机制。
纳入 40 例经治疗的贲门失弛缓症患者(平均年龄 52.9 岁;27 例[68%]为男性),其中 20 例有反流症状(RS+;胃食管反流病问卷[GORDQ]≥8),20 例无反流症状(RS-:GORDQ<8)。患者接受食管胃结合部扩张性、高分辨率测压、定时钡餐食管造影、24 小时 pH-阻抗监测(抑酸后)和食管酸灌注及扩张感知。通过内镜评估食管炎的存在。
24 小时 pH-阻抗监测的总酸暴露时间在有(RS+)和无(RS-)反流症状的患者之间无显著差异。在 RS+患者中,酸发酵高于 RS-患者(RS+:6.6%(95%CI 2.96% 至 10.2%)比 RS-:1.8%(95%CI -0.45% 至 4.1%,p=0.03),且酸反流清除延迟(RS+:6%(95%CI 0.94% 至 11%)比 RS-:3.4%(95%CI -0.34% 至 7.18%),p=0.051)。RS+和 RS-两组的反流症状均与酸无关,反映为较低的症状指数。RS+患者对酸高度敏感,出现烧心的时间明显缩短(RS+:4(2-6)比 RS-:30(14-30)min,p<0.001),症状强度明显更高(RS+:7(4.8-9)比 RS-:0.5(0-4.5)视觉模拟评分,p<0.001)在酸灌注期间。他们对机械刺激的阈值也较低。
治疗后贲门失弛缓症患者的反流症状很少由胃食管反流引起,大多数食管酸化与反流无关。相反,治疗后出现反流症状的贲门失弛缓症患者表现出对化学和机械刺激的食管高敏感性,这可能决定了症状的产生。