Holmberg C, Perheentupa J, Launiala K, Hallman N
Arch Dis Child. 1977 Apr;52(4):255-67. doi: 10.1136/adc.52.4.255.
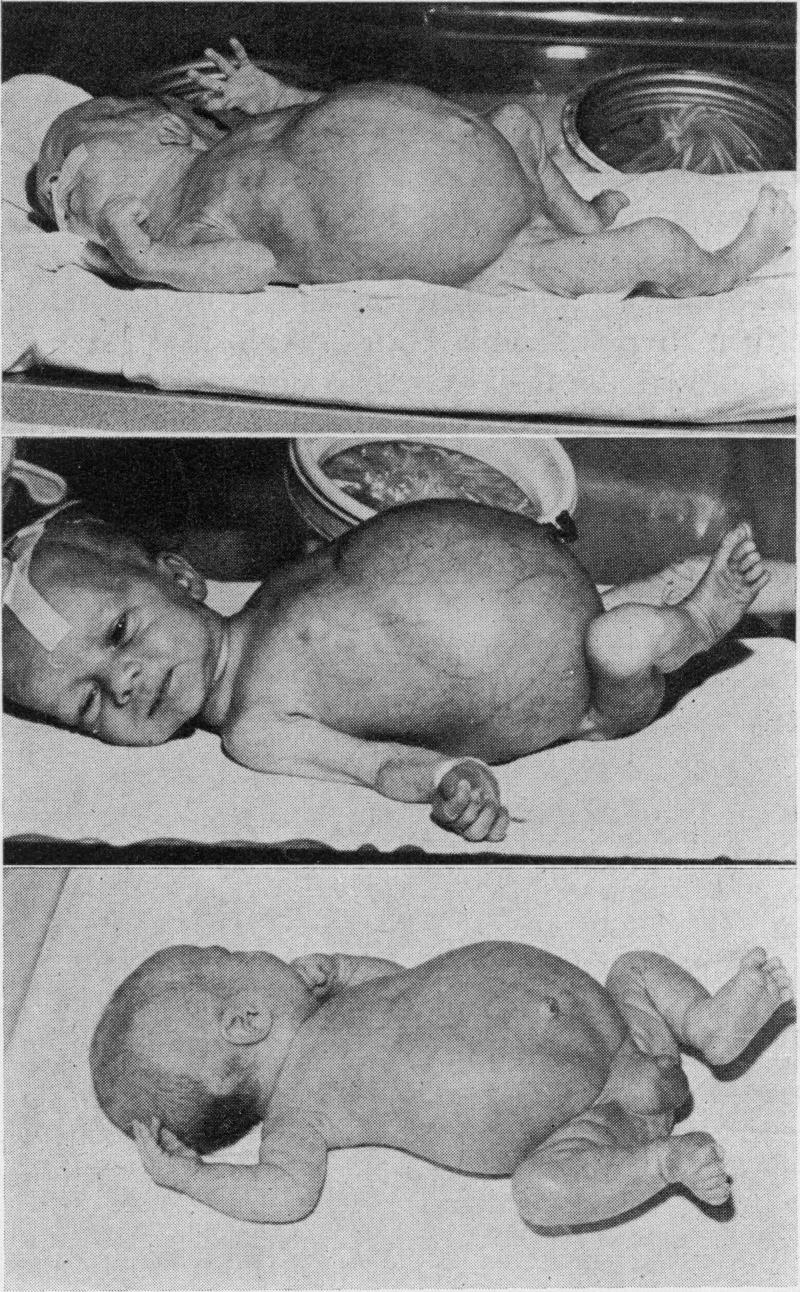
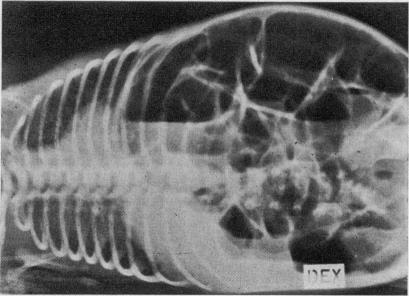
Clinical findings in 21 Finnish children with congenital chloride diarrhoea are reported. Inheritance of this disease by the autosomal recessive mode is established. All children were born 1-8 weeks prematurely. Hydramnios was present in every case and no meconium was observed; intrauterine onset of diarrhoea is thus apparent. In most cases the diarrhoea or passing of large volumes of "urine" was noted on the first day of life and the abdomen was usually large and distended. The neonatla weight loss was abnormally large, and was associated with hypochloraemia and hyponatraemia. Some infants survived the neonatal period without adequate therapy. They presented later with failure to thrive and usually had hypochloraemia, hypokalaemia, and metabolic alkalosis associated with hyperaldosteronism. However, these features may be absent and the diagnosis is based on a history of hydramnios and diarrhoea, and a faecal Cl- concentration which always exceeds 90 mmol/l when fluid and electrolyte deficits have been corrected. Lower faecal Cl- concentrations were seen only in chronic hypochloraemia, which is also associated with achloriduria. Adequate treatment consists of full continuous replacement of the faecal losses of water, NaCl, and KCl. This should be given intravenously in the early neonatal period; later a solution can be taken orally with meals. The dose has to be adjusted to maintain normal serum electrolyte concentrations, normal blood pH, and some chloriduria. This therapy prevents the renal lesions and the retarded growth and psychomotor development which were seen in the children who were diagnosed late and in those who received inadequate replacement therapy. The watery diarrhoea persists and increases slightly with age, though patients learn to live with their disease and to make an adequate social adjustment.
本文报告了21例芬兰先天性氯腹泻患儿的临床发现。已确定该疾病为常染色体隐性遗传模式。所有患儿均早产1 - 8周。每例患儿均有羊水过多,未观察到胎粪;因此,腹泻在子宫内即已开始。多数情况下,出生第一天即出现腹泻或排出大量“尿液”,腹部通常膨隆。新生儿体重下降异常大,且伴有低氯血症和低钠血症。部分婴儿未经充分治疗存活至新生儿期后,出现生长发育迟缓,通常伴有低氯血症、低钾血症及与醛固酮增多症相关的代谢性碱中毒。然而,这些特征可能并不存在,诊断依据为羊水过多和腹泻病史,以及在纠正液体和电解质缺乏后粪便氯浓度始终超过90 mmol/L。仅在慢性低氯血症(也与无氯尿症相关)中观察到较低的粪便氯浓度。充分治疗包括持续完全补充粪便中丢失的水分、氯化钠和氯化钾。在新生儿早期应静脉给予;之后可随餐口服溶液。必须调整剂量以维持正常的血清电解质浓度、正常的血液pH值及一定程度的尿氯排泄。这种治疗可预防肾脏病变以及生长发育迟缓和精神运动发育迟缓,这些情况见于诊断较晚及接受替代治疗不足的患儿。水样腹泻持续存在,并随年龄略有增加,不过患者学会了与疾病共处并进行适当的社会适应。