Heart and Vascular Center, Semmelweis University, Városmajor Street 68, Budapest, 1122, Hungary.
Cardiovasc Intervent Radiol. 2020 Aug;43(8):1134-1142. doi: 10.1007/s00270-020-02522-5. Epub 2020 May 21.
In the absence of literature data, we aimed to determine the long-term patency rates of middle/distal common carotid artery (CCA) stenting and to investigate predisposing factors in the development of in-stent restenosis (ISR).
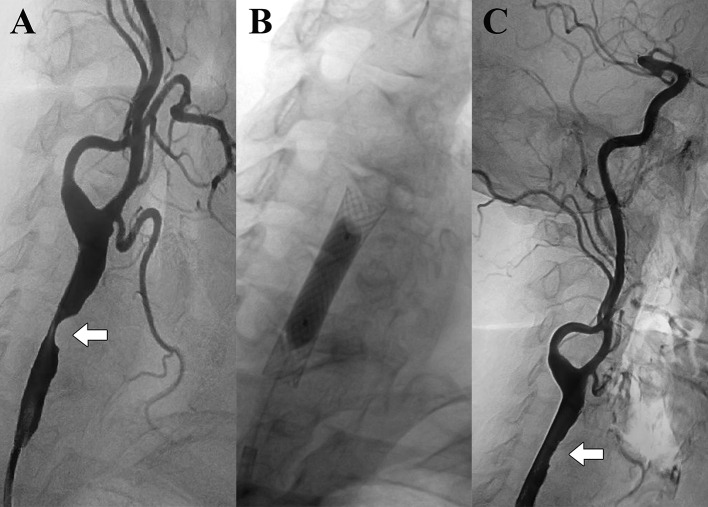
Fifty-one patients (30 males, median age 63.5 years), who underwent stenting with 51 self-expandable stents for significant (≥ 60%) stenosis of the middle/distal CCA, were analyzed retrospectively. Patient (atherosclerotic risk factors, comorbidities, medications), vessel (elongation), lesion (stenosis grade, length, calcification, location), and stent characteristics (material, diameter, length, fracture) were examined. Duplex ultrasonography was used to monitor stent patency. The Mann-Whitney U and Fisher's exact tests, Kaplan-Meier analyses, and a log-rank test were used statistically.
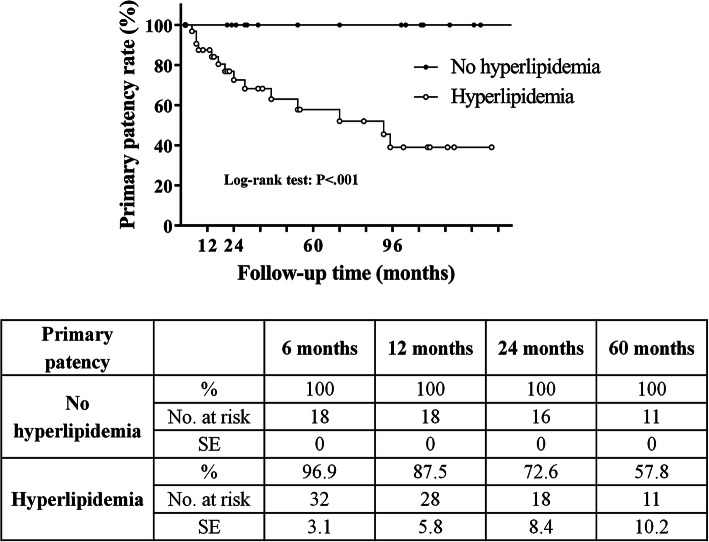
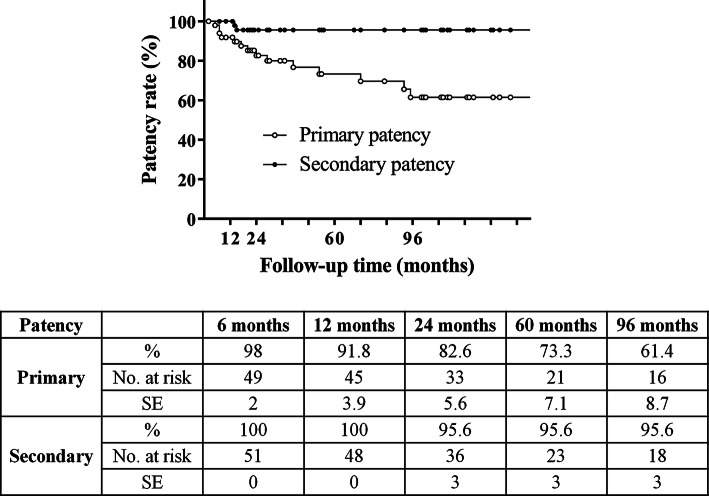
The median follow-up time was 35 months (interquartile range, 20-102 months). Significant (≥ 70%) ISR developed in 14 patients (27.5%; stenosis, N = 10; entire CCA occlusion, N = 4). Primary patency rates were 98%, 92%, 83%, 73%, and 61% at 6, 12, 24, 60, and 96 months, respectively. Reintervention was performed in six patients (11.8%) with nonocclusive ISR. Secondary patency rates were 100% at 6 and 12 months and 96% at 24, 60, and 96 months. In-stent restenosis developed more frequently (P < .001) in patients with hyperlipidemia; primary patency rates were also significantly worse (Chi-square, 11.08; degrees of freedom, 1; P < .001) in patients with hyperlipidemia compared to those without.
Stenting of the middle/distal CCA can be performed with acceptable patency rates. If intervention is unequivocally needed, patients with hyperlipidemia will require closer follow-up care.
Level 3, Local non-random sample.
由于缺乏文献数据,我们旨在确定中/远端颈总动脉(CCA)支架置入术的长期通畅率,并探讨支架内再狭窄(ISR)发生的相关因素。
回顾性分析了 51 例(30 例男性,中位年龄 63.5 岁)因中/远端 CCA 狭窄程度≥60%而行支架置入术的患者,共置入 51 枚自膨式支架。分析患者(动脉粥样硬化危险因素、合并症、药物使用情况)、血管(长度)、病变(狭窄程度、长度、钙化、位置)和支架特征(材料、直径、长度、断裂)。采用超声检查监测支架通畅情况。采用 Mann-Whitney U 检验、Fisher 确切概率法、Kaplan-Meier 分析和对数秩检验进行统计学分析。
中位随访时间为 35 个月(四分位间距 20-102 个月)。14 例(27.5%;狭窄 10 例,整个 CCA 闭塞 4 例)患者出现明显(≥70%)ISR。6、12、24、60 和 96 个月时,初始通畅率分别为 98%、92%、83%、73%和 61%。6 例(11.8%)非闭塞性 ISR 患者行再次介入治疗。6 个月和 12 个月时,次级通畅率为 100%;24、60 和 96 个月时,次级通畅率为 96%。支架内再狭窄在高脂血症患者中更常见(P<0.001),并且在高脂血症患者中,初始通畅率也显著更差(卡方检验,11.08;自由度,1;P<0.001)。
中/远端 CCA 支架置入术具有可接受的通畅率。如果需要进行干预,高脂血症患者需要更密切的随访。
3 级,局部非随机样本。