Metabolic Research Laboratories and MRC Metabolic Diseases Unit, Wellcome Trust-MRC Institute of Metabolic Science, University of Cambridge, Cambridge, United Kingdom.
Department of Obstetrics and Gynaecology, the Rosie Hospital and NIHR Cambridge Comprehensive Biomedical Research Centre, University of Cambridge, Cambridge, United Kingdom.
PLoS Med. 2020 May 22;17(5):e1003126. doi: 10.1371/journal.pmed.1003126. eCollection 2020 May.
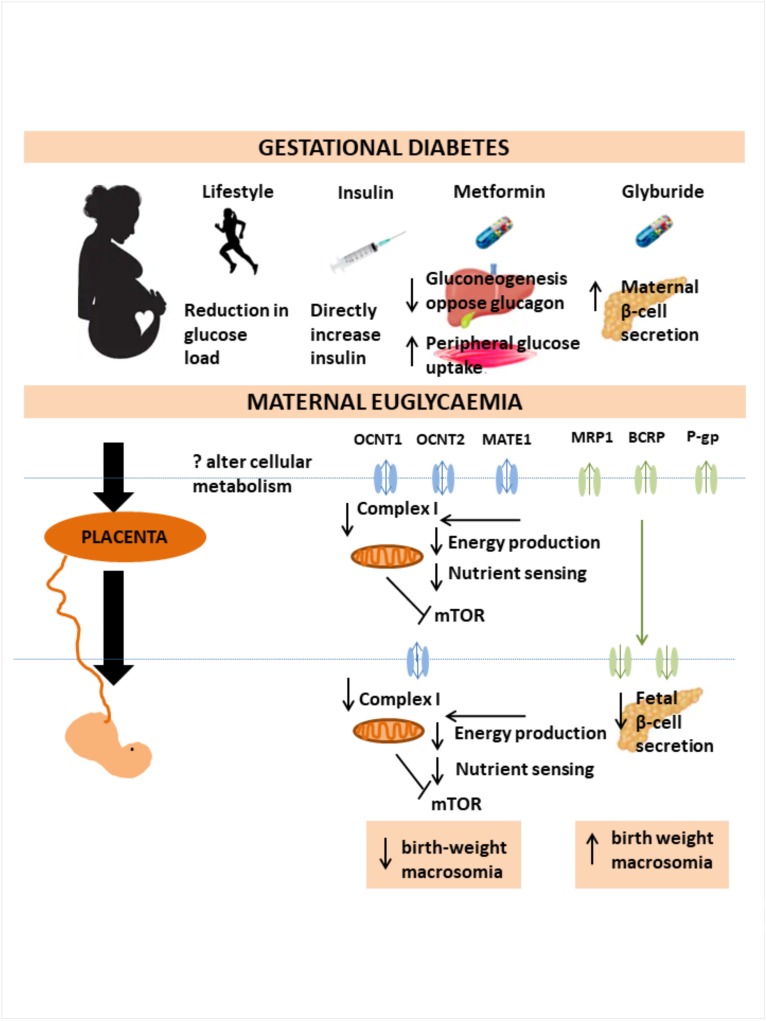
Fetal growth in gestational diabetes mellitus (GDM) is directly linked to maternal glycaemic control; however, this relationship may be altered by oral anti-hyperglycaemic agents. Unlike insulin, such drugs cross the placenta and may thus have independent effects on fetal or placental tissues. We investigated the association between GDM treatment and fetal, neonatal, and childhood growth.
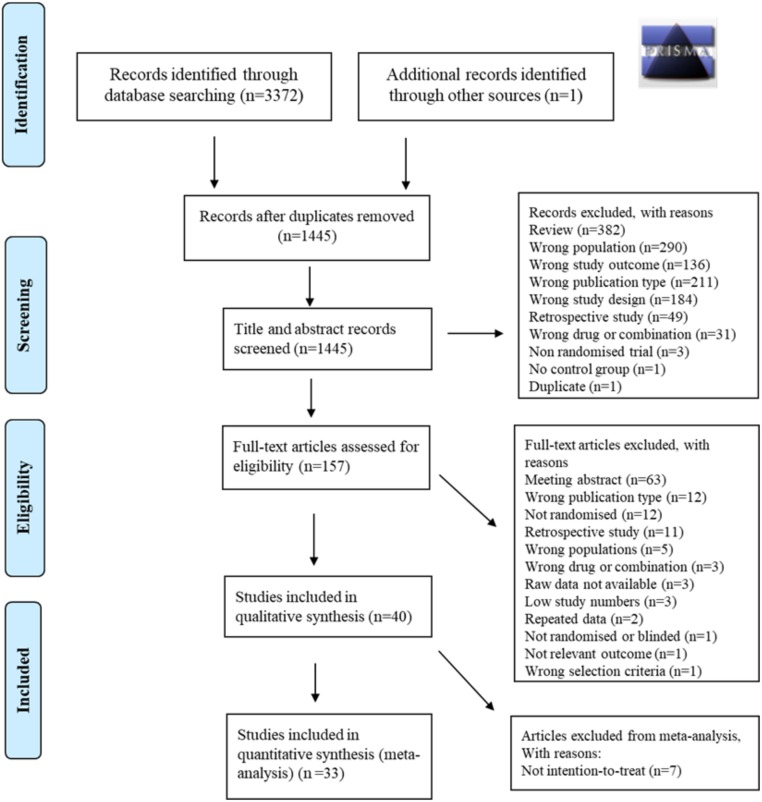
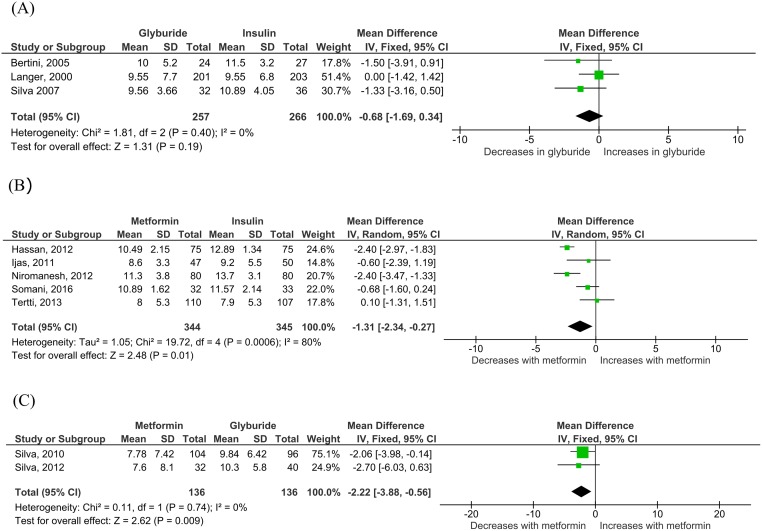
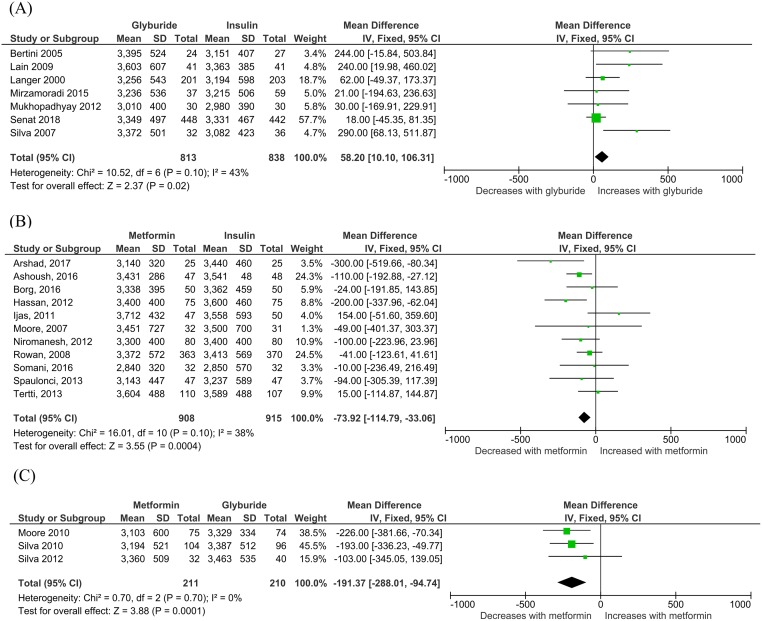
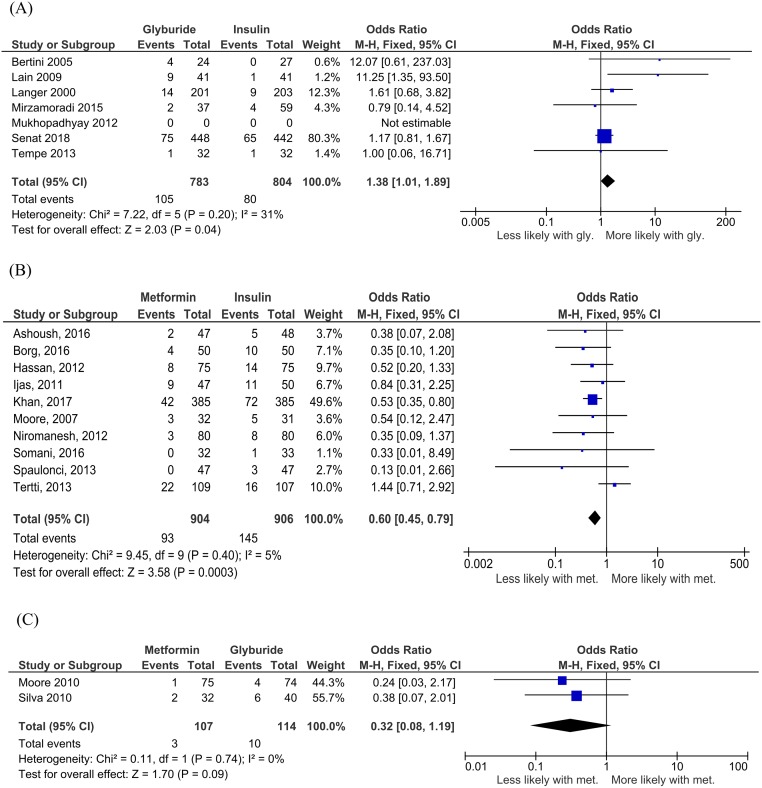
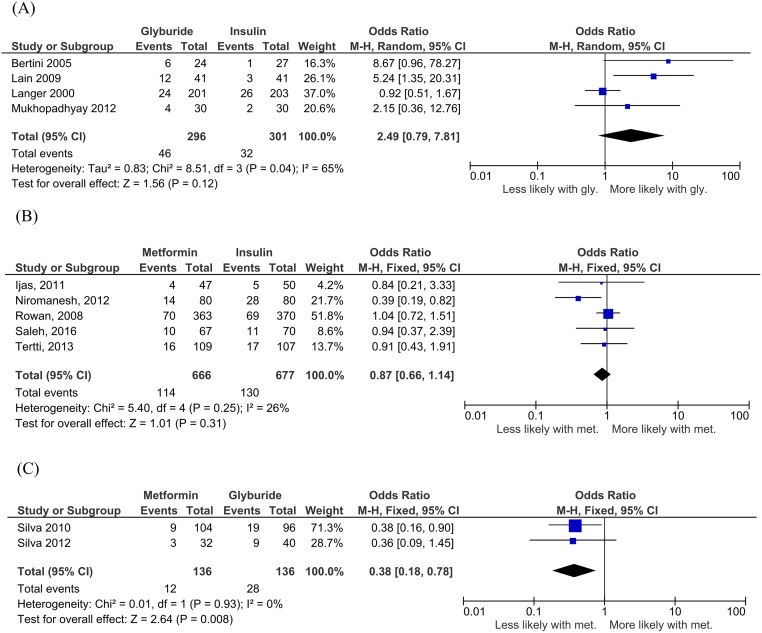
PubMed, Ovid Embase, Medline, Web of Science, ClinicalTrials.gov, and Cochrane databases were systematically searched (inception to 12 February 2020). Outcomes of GDM-affected pregnancies randomised to treatment with metformin, glyburide, or insulin were included. Studies including preexisting diabetes or nondiabetic women were excluded. Two reviewers independently assessed eligibility and risk of bias, with conflicts resolved by a third reviewer. Maternal outcome measures were glycaemic control, weight gain, and treatment failure. Offspring anthropometric parameters included fetal, neonatal, and childhood weight and body composition data. Thirty-three studies (n = 4,944), from geographical locations including Europe, North Africa, the Middle East, Asia, Australia/New Zealand, and the United States/Latin America, met eligibility criteria. Twenty-two studies (n = 2,801) randomised women to metformin versus insulin, 8 studies (n = 1,722) to glyburide versus insulin, and 3 studies (n = 421) to metformin versus glyburide. Eleven studies (n = 2,204) reported maternal outcomes. No differences in fasting blood glucose (FBS), random blood glucose (RBS), or glycated haemoglobin (HbA1c) were reported. No studies reported fetal growth parameters. Thirty-three studies (n = 4,733) reported birth weight. Glyburide-exposed neonates were heavier at birth (58.20 g, 95% confidence interval [CI] 10.10-106.31, p = 0.02) with increased risk of macrosomia (odds ratio [OR] 1.38, 95% CI 1.01-1.89, p = 0.04) versus neonates of insulin-treated mothers. Metformin-exposed neonates were born lighter (-73.92 g, 95% CI -114.79 to -33.06 g, p < 0.001) with reduced risk of macrosomia (OR 0.60, 95% CI 0.45-0.79, p < 0.001) than insulin-exposed neonates. Metformin-exposed neonates were born lighter (-191.73 g, 95% CI -288.01 to -94.74, p < 0.001) with a nonsignificant reduction in macrosomia risk (OR 0.32, 95% CI 0.08-1.19, I2 = 0%, p = 0.09) versus glyburide-exposed neonates. Glyburide-exposed neonates had a nonsignificant increase in total fat mass (103.2 g, 95% CI -3.91 to 210.31, p = 0.06) and increased abdominal (0.90 cm, 95% CI 0.03-1.77, p = 0.04) and chest circumferences (0.80 cm, 95% CI 0.07-1.53, p = 0.03) versus insulin-exposed neonates. Metformin-exposed neonates had decreased ponderal index (-0.13 kg/m3, 95% CI -0.26 to -0.00, p = 0.04) and reduced head (-0.21, 95% CI -0.39 to -0.03, p = 0.03) and chest circumferences (-0.34 cm, 95% CI -0.62 to -0.05, p = 0.02) versus the insulin-treated group. Metformin-exposed neonates had decreased ponderal index (-0.09 kg/m3, 95% CI -0.17 to -0.01, p = 0.03) versus glyburide-exposed neonates. Study limitations include heterogeneity in dosing, heterogeneity in GDM diagnostic criteria, and few studies reporting longitudinal growth outcomes.
Maternal randomisation to glyburide resulted in heavier neonates with a propensity to increased adiposity versus insulin- or metformin-exposed groups. Metformin-exposed neonates were lighter with reduced lean mass versus insulin- or glyburide-exposed groups, independent of maternal glycaemic control. Oral anti-hyperglycaemics cross the placenta, so effects on fetal anthropometry could result from direct actions on the fetus and/or placenta. We highlight a need for further studies examining the effects of intrauterine exposure to antidiabetic agents on longitudinal growth, and the importance of monitoring fetal growth and maternal glycaemic control when treating GDM. This review protocol was registered with PROSPERO (CRD42019134664/CRD42018117503).
妊娠糖尿病(GDM)中的胎儿生长与母体血糖控制直接相关;然而,这种关系可能因口服抗高血糖药物而改变。与胰岛素不同,这些药物可以穿过胎盘,因此可能对胎儿或胎盘组织产生独立的影响。我们研究了 GDM 治疗与胎儿、新生儿和儿童生长的关系。
系统地检索了 PubMed、Ovid Embase、Medline、Web of Science、ClinicalTrials.gov 和 Cochrane 数据库(从成立到 2020 年 2 月 12 日)。纳入了接受二甲双胍、格列本脲或胰岛素治疗的 GDM 孕妇的妊娠结局。排除了包括既往糖尿病或非糖尿病女性的研究。两名审查员独立评估了合格性和偏倚风险,通过第三名审查员解决了冲突。母体结局测量指标包括血糖控制、体重增加和治疗失败。胎儿体重、新生儿体重和儿童体重和身体成分数据等胎儿生长参数。来自欧洲、北非、中东、亚洲、澳大利亚/新西兰和美国/拉丁美洲等地理位置的 33 项研究(n=4944)符合入选标准。22 项研究(n=2801)将女性随机分配至二甲双胍与胰岛素组,8 项研究(n=1722)将格列本脲与胰岛素组,3 项研究(n=421)将二甲双胍与格列本脲组。11 项研究(n=2204)报告了母体结局。空腹血糖(FBS)、随机血糖(RBS)或糖化血红蛋白(HbA1c)无差异。没有研究报告胎儿生长参数。33 项研究(n=4733)报告了出生体重。与胰岛素治疗的母亲所生的新生儿相比,格列本脲暴露的新生儿出生时体重更重(58.20 g,95%置信区间 [CI] 10.10-106.31,p=0.02),且巨大儿的风险增加(比值比 [OR] 1.38,95%CI 1.01-1.89,p=0.04)。二甲双胍暴露的新生儿出生时体重较轻(-73.92 g,95%CI-114.79 至-33.06 g,p<0.001),且巨大儿的风险降低(OR 0.60,95%CI 0.45-0.79,p<0.001)。与胰岛素暴露的新生儿相比,格列本脲暴露的新生儿出生时体重更轻(-191.73 g,95%CI-288.01 至-94.74,p<0.001),且巨大儿的风险降低(OR 0.32,95%CI 0.08-1.19,I2=0%,p=0.09)。与胰岛素暴露的新生儿相比,格列本脲暴露的新生儿总脂肪量增加(103.2 g,95%CI-3.91 至 210.31,p=0.06),腹部(0.90 cm,95%CI 0.03-1.77,p=0.04)和胸部(0.80 cm,95%CI 0.07-1.53,p=0.03)周长增加。与胰岛素治疗的新生儿相比,二甲双胍暴露的新生儿体重指数(ponderal index)降低(-0.13 kg/m3,95%CI-0.26 至-0.00,p=0.04),头部(-0.21,95%CI-0.39 至-0.03,p=0.03)和胸部周长(-0.34 cm,95%CI-0.62 至-0.05,p=0.02)减小。与格列本脲暴露的新生儿相比,二甲双胍暴露的新生儿体重指数(ponderal index)降低(-0.09 kg/m3,95%CI-0.17 至-0.01,p=0.03)。研究局限性包括剂量异质性、GDM 诊断标准异质性以及报告纵向生长结局的研究较少。
与胰岛素或二甲双胍相比,母体随机接受格列本脲治疗会导致新生儿体重增加,且倾向于增加脂肪量。与胰岛素或格列本脲相比,二甲双胍暴露的新生儿体重较轻,且与胰岛素或格列本脲相比,瘦体重减少,而与母体血糖控制无关。口服抗高血糖药物可以穿过胎盘,因此对胎儿形态的影响可能是由于直接作用于胎儿和/或胎盘。我们强调需要进一步研究宫内暴露于抗糖尿病药物对纵向生长的影响,以及在治疗 GDM 时监测胎儿生长和母体血糖控制的重要性。本综述方案已在 PROSPERO(CRD42019134664/CRD42018117503)注册。