Department of Clinical Therapeutics, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece.
Faculty of Freiburg, Hematology and Oncology Department, Interdisciplinary Cancer Center (ITZ) and Comprehensive Cancer Center Freiburg (CCCF), University of Freiburg, Freiburg, Germany.
Leukemia. 2020 Aug;34(8):2000-2011. doi: 10.1038/s41375-020-0876-z. Epub 2020 May 22.
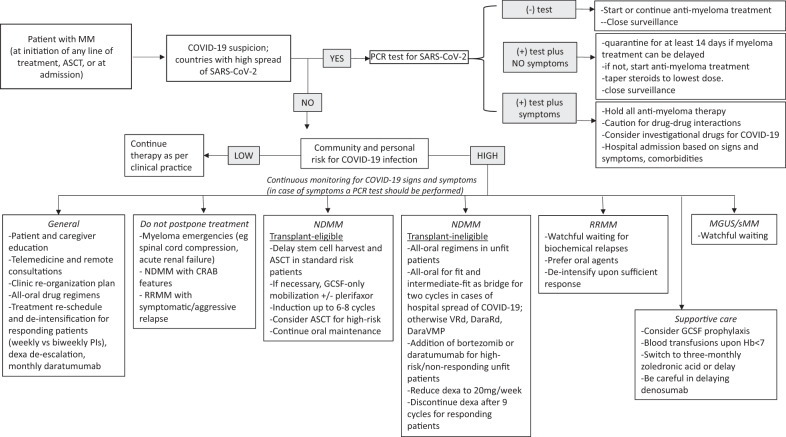
Patients with multiple myeloma (MM) seem to be at increased risk for more severe COVID-19 infection and associated complications due to their immunocompromised state, the older age and comorbidities. The European Myeloma Network has provided an expert consensus statement in order to guide therapeutic decisions in the era of the COVID-19 pandemic. Patient education for personal hygiene and social distancing measures, along with treatment individualization, telemedicine and continuous surveillance for early diagnosis of COVID-19 are essential. In countries or local communities where COVID-19 infection is widely spread, MM patients should have a PCR test of nasopharyngeal swab for SARS-CoV-2 before hospital admission, starting a new treatment line, cell apheresis or ASCT in order to avoid ward or community spread and infections. Oral agent-based regimens should be considered, especially for the elderly and frail patients with standard risk disease, whereas de-intensified regimens for dexamethasone, bortezomib, carfilzomib and daratumumab should be used based on patient risk and response. Treatment initiation should not be postponed for patients with end organ damage, myeloma emergencies and aggressive relapses. Autologous (and especially allogeneic) transplantation should be delayed and extended induction should be administered, especially in standard risk patients and those with adequate MM response to induction. Watchful waiting should be considered for standard risk relapsed patients with low tumor burden, and slow biochemical relapses. The conduction of clinical trials should continue with appropriate adaptations to the current circumstances. Patients with MM and symptomatic COVID-19 disease should interrupt anti-myeloma treatment until recovery. For patients with positive PCR test for SARS-CoV-2, but with no symptoms for COVID-19, a 14-day quarantine should be considered if myeloma-related events allow the delay of treatment. The need for surveillance for drug interactions due to polypharmacy is highlighted. The participation in international COVID-19 cancer registries is greatly encouraged.
多发性骨髓瘤(MM)患者由于免疫功能低下、年龄较大和合并症,似乎面临着更严重的 COVID-19 感染和相关并发症的风险增加。欧洲骨髓瘤网络(European Myeloma Network)提供了一份专家共识声明,以指导 COVID-19 大流行时代的治疗决策。对患者进行个人卫生和社会隔离措施的教育,以及治疗个体化、远程医疗和对 COVID-19 的早期诊断进行持续监测至关重要。在 COVID-19 感染广泛传播的国家或当地社区,MM 患者在入院前、开始新的治疗线、细胞分离术或 ASCT 之前,应进行鼻咽拭子 SARS-CoV-2 的 PCR 检测,以避免病房或社区传播和感染。应考虑使用基于口服药物的方案,特别是对于患有标准风险疾病的老年和体弱患者,而应根据患者的风险和反应使用地塞米松、硼替佐米、卡非佐米和达雷妥尤单抗的减量化方案。对于有终末器官损害、骨髓瘤急症和侵袭性复发的患者,不应推迟治疗开始。应推迟自体(尤其是异体)移植,并应给予延长诱导期,特别是在标准风险患者和那些对诱导有足够 MM 反应的患者中。对于标准风险复发、肿瘤负荷低和生化缓慢复发的患者,应考虑观察等待。应继续进行临床试验,同时适当适应当前情况。患有 MM 和有症状 COVID-19 疾病的患者应中断抗骨髓瘤治疗,直至康复。对于 SARS-CoV-2 PCR 检测呈阳性但无 COVID-19 症状的患者,如果骨髓瘤相关事件允许延迟治疗,则应考虑 14 天的隔离。强调了因多药治疗而需要监测药物相互作用的问题。鼓励患者积极参与国际 COVID-19 癌症登记处。