OCM | Orthopädische Chirurgie München, Steinerstrasse 6, 812306, München, Germany.
St. Joseph Krankenhaus, Regensburg, Germany.
Arch Orthop Trauma Surg. 2020 Oct;140(10):1437-1444. doi: 10.1007/s00402-020-03476-6. Epub 2020 May 23.
High tibial osteotomy (HTO) for varus deformities is a common concomitant treatment in cartilage surgery. Aim of the present study was to analyze factors influencing the decision towards accompanying HTO in patients with cartilage defects of the medial femoral condyle, such as the amount of varus deformity.
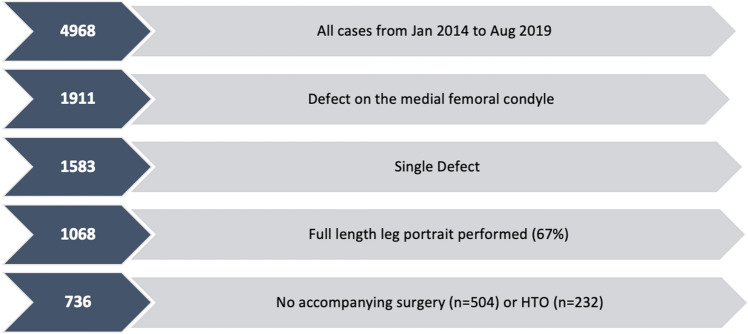
Data from 4986 patients treated for cartilage defects of the knee from the German Cartilage Registry (KnorpelRegister DGOU) were used for the current analysis. Seven hundred and thirty-six patients fulfilled the inclusion criteria. Their data were analyzed for factors influencing the decision towards performing a concomitant HTO using t test, univariate and multivariate binary logistic regression models.
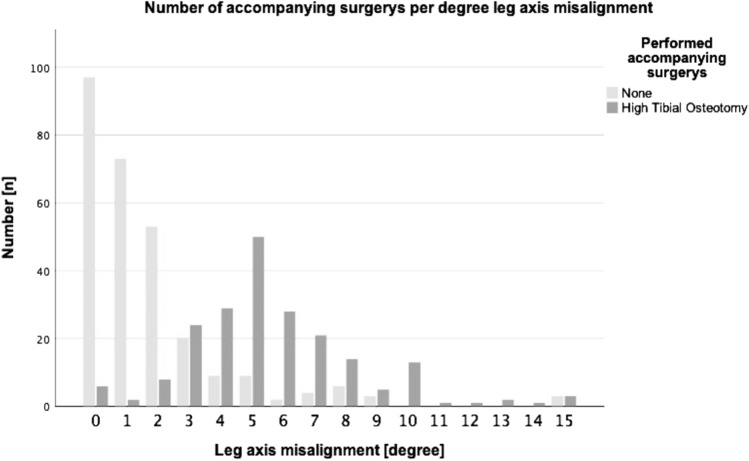
The break point at which the majority of patients receive a concomitant HTO is 3° of varus deformity. Several factors apart from the amount of varus deformity (5.61 ± 2.73° vs. 1.72 ± 2.38°, p < 0.00) differed significantly between the group of patients with HTO and those without. These included defect size (441.6 ± 225.3 mm vs. 386.5 ± 204.2 mm, p = 0.001), symptom duration (29.53 ± 44.58 months vs. 21.85 ± 34.17 months, p = 0.021), defect grade (62.5% IVa/IVb vs. 57.3% IVa/IVb, p = 0.014), integrity of corresponding joint surface (10.8% grade III-IV vs. 0.2% grade III-IV, p < 0.001), meniscus status (15.5% > 1/3 resected vs. 4.4% > 1/3 resected, p < 0.001) and number of previous surgeries (1.01 ± 1.06 vs. 0.75 ± 1.00, p = 0.001). In the stepwise multivariate binary logistic regression test, only the amount of varus deformity, symptom duration and quality of the corresponding joint surface remained significant predictors associated with performing a concomitant HTO.
Based upon data from a nationwide cohort, additional HTO in context with cartilage repair procedures of the medial femoral condyle is frequently performed even in mild varus deformities less than 5°. Other factors also seem to influence decision for HTO.
胫骨高位截骨术(HTO)治疗内翻畸形是软骨手术的常见伴随治疗。本研究的目的是分析影响内侧股骨髁软骨缺损患者行伴随 HTO 决策的因素,如内翻畸形的程度。
本研究使用了德国软骨注册处(KnorpelRegister DGOU)的 4986 例膝关节软骨缺损患者的数据。736 例患者符合纳入标准。使用 t 检验、单变量和多变量二项逻辑回归模型对影响伴随 HTO 决策的因素进行分析。
大多数患者接受伴随 HTO 的转折点是 3°内翻畸形。除了内翻畸形的程度(5.61±2.73°与 1.72±2.38°,p<0.00)之外,HTO 组和非 HTO 组之间的其他几个因素差异有统计学意义。这些因素包括缺损大小(441.6±225.3mm 与 386.5±204.2mm,p=0.001)、症状持续时间(29.53±44.58 个月与 21.85±34.17 个月,p=0.021)、缺损分级(62.5%IVa/IVb 与 57.3%IVa/IVb,p=0.014)、相应关节面的完整性(10.8%III-IV 级与 0.2%III-IV 级,p<0.001)、半月板状态(15.5%>1/3 切除与 4.4%>1/3 切除,p<0.001)和既往手术次数(1.01±1.06 与 0.75±1.00,p=0.001)。在逐步多变量二项逻辑回归检验中,只有内翻畸形的程度、症状持续时间和相应关节面的质量仍然是与伴随 HTO 相关的显著预测因素。
基于全国性队列的数据,即使是在小于 5°的轻度内翻畸形中,内侧股骨髁软骨修复术中也经常需要额外的 HTO。其他因素似乎也会影响 HTO 的决策。