Goodnight Family Department of Sustainable Development, Appalachian State University, Boone, NC, United States of America.
Center for Vaccine Innovation and Access, PATH, Seattle, WA, United States of America.
PLoS One. 2020 May 29;15(5):e0232941. doi: 10.1371/journal.pone.0232941. eCollection 2020.
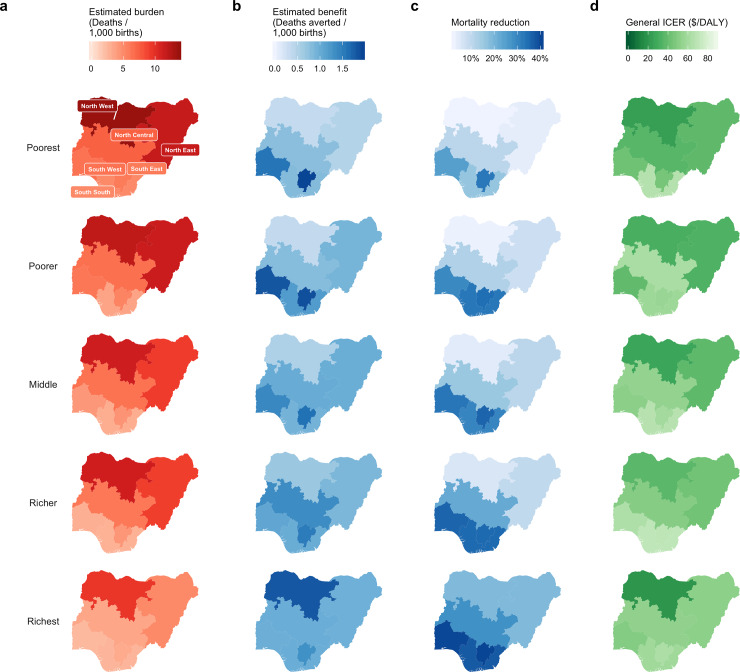
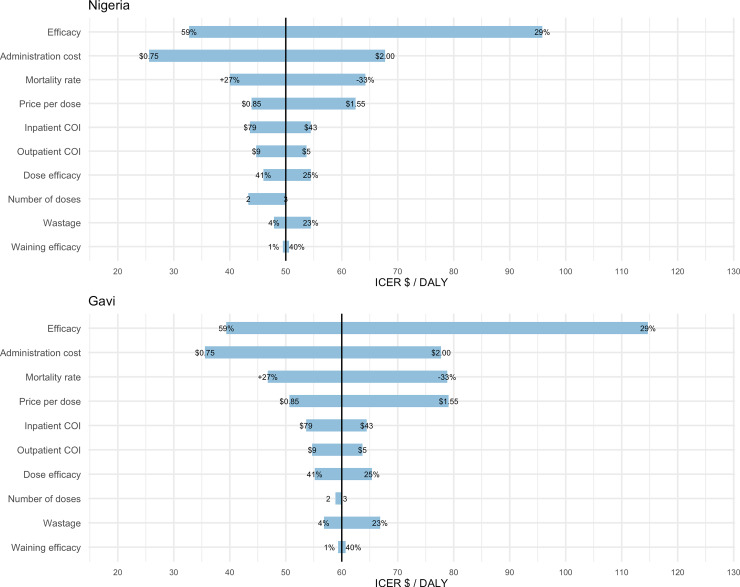
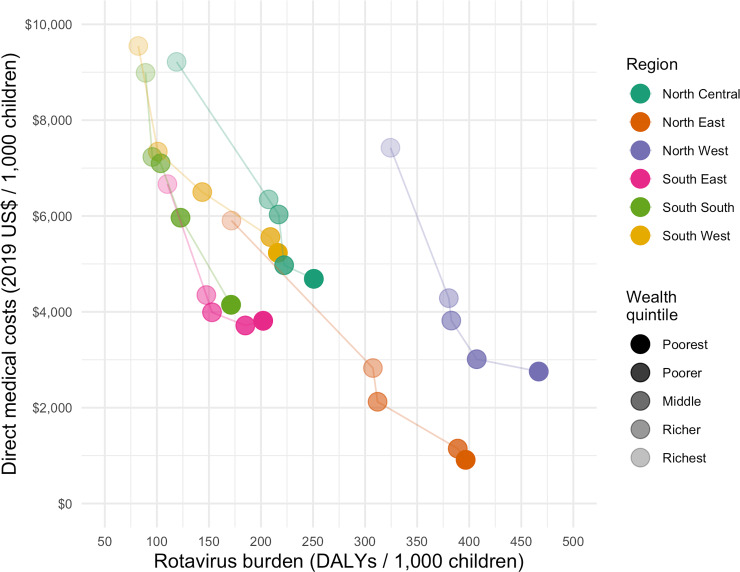
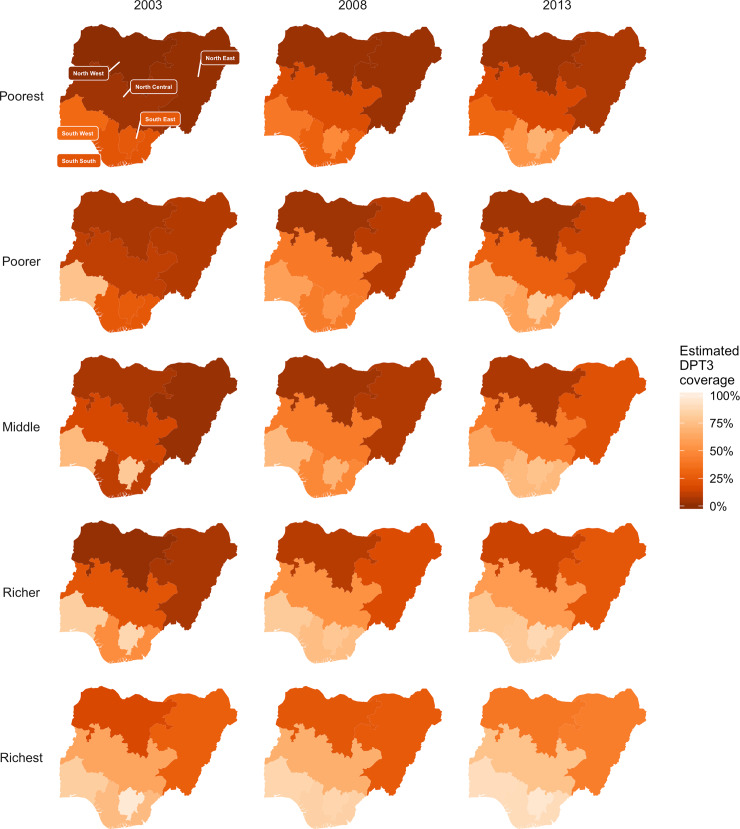
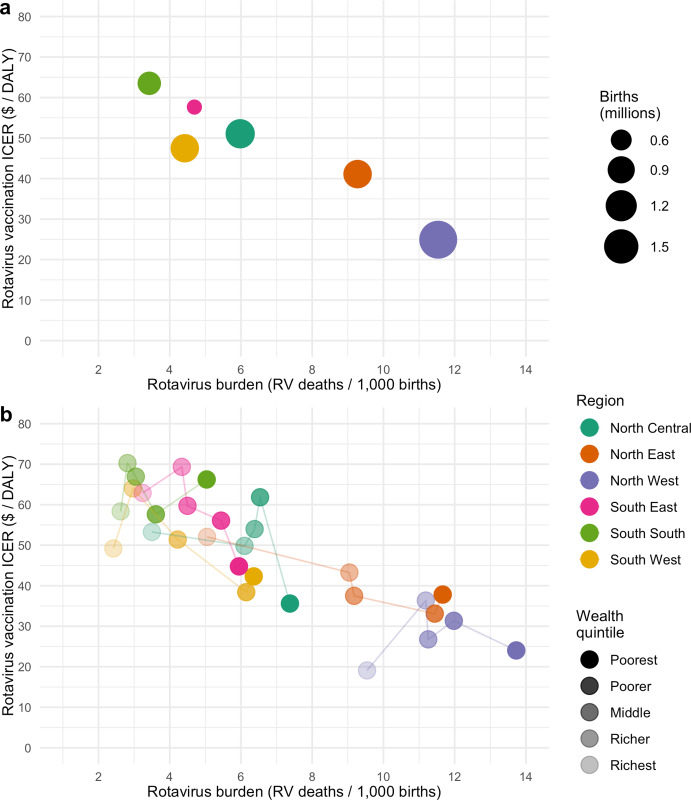
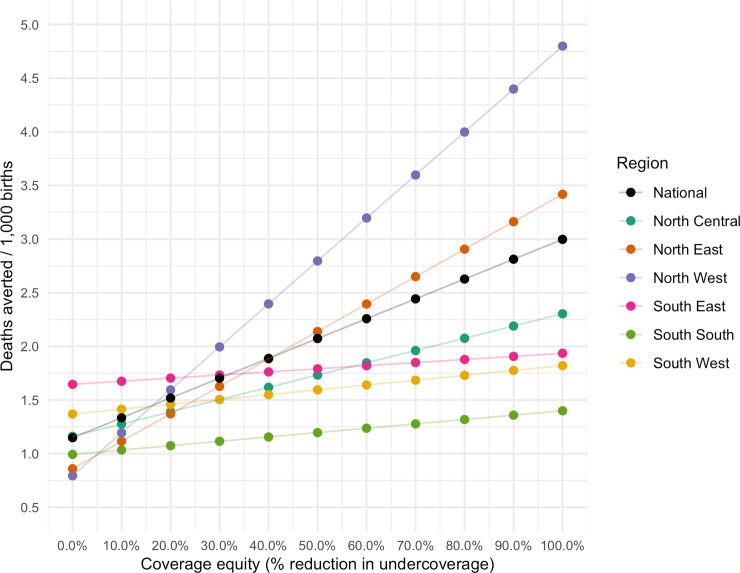
Child mortality from rotavirus gastroenteritis remains high in Nigeria, representing 14% of all rotavirus deaths worldwide. Here, we examine the potential impact and cost-effectiveness of national rotavirus vaccine introduction in geographic and economic subpopulations of Nigeria. We projected the health and economic outcomes of rotavirus vaccination in children over the first five years of life using a spreadsheet-based model. We modeled child populations using national survey data on rotavirus mortality risk factors and vaccination coverage to predict burden and impact across regional and wealth quintile subpopulations within Nigeria. Our base case considered introduction of a general rotavirus vaccine, modeled to encompass characteristics of existing vaccines, versus no vaccine. Base case costs were estimated from the government perspective, assuming Gavi subsidies, over the first five years. We also present estimates from the cost of vaccination from the perspective of Gavi. We explored uncertainty in model parameters through probabilistic uncertainty, one-way sensitivity, and scenario analyses. According to our estimates, rotavirus enteritis was responsible for 47,898 [95% Uncertainty Limits: 35,361; 63,703] child deaths per year, with approximately 80% of the national burden concentrated in the three northern regions of Nigeria. Rotavirus vaccination was estimated to prevent 6,454 [3,960; 9,721] deaths, 13% [9%; 18%] of the national annual RV burden. National ICERs for rotavirus vaccination from the Nigerian government and Gavi perspectives were US$47 [$18; $105] and $62 [$29; $130] per DALY averted, respectively. General rotavirus vaccination was projected to reduce rotavirus mortality by only 6% [4%; 9%] in the North West region compared to 35% [24%; 47%] in the South East region. Base case ICERs ranged from US$25 [10; 56] per DALY averted in North West to US$64 [18; 157] per DALY averted in South South. Gavi perspective ICERs ranged from US$33 [$15; $68] in North West to US$88 [35; 191] per DALY averted in South South. According to one-way sensitivity analyses, ICERs were most sensitive to vaccine efficacy, followed by estimated administrative costs and rotavirus mortality. Disparities in mortality reduction were largely driven by inequality in vaccination coverage across regions and between socioeconomic subpopulations. Due to high, persistent, and inequitable burden of rotavirus in Nigeria, routine vaccination with any of these rotavirus vaccines would be an high impact and cost-effective strategy in reducing child mortality.
在尼日利亚,轮状病毒肠胃炎导致的儿童死亡率仍然很高,占全球所有轮状病毒死亡人数的 14%。在这里,我们研究了在尼日利亚的地理和经济亚人群中引入国家轮状病毒疫苗的潜在影响和成本效益。我们使用基于电子表格的模型预测了儿童在生命的头五年中接种轮状病毒疫苗的健康和经济结果。我们使用国家调查数据来预测轮状病毒死亡率风险因素和疫苗接种覆盖率,以预测尼日利亚各地区和财富五分位数亚人群的负担和影响。我们的基本情况考虑了引入一种通用的轮状病毒疫苗,该疫苗被建模为包含现有疫苗的特征,而不是不接种疫苗。基本情况成本是从政府的角度估计的,假设 Gavi 补贴,在头五年内。我们还从 Gavi 的角度介绍了接种疫苗的成本估算。我们通过概率不确定性、单向敏感性和情景分析来探索模型参数的不确定性。根据我们的估计,轮状病毒肠炎每年导致 47898 例[95%不确定性范围:35361;63703]儿童死亡,全国约 80%的负担集中在尼日利亚的三个北部地区。轮状病毒疫苗接种估计可预防 6454 例[3,960;9721]死亡,占全国年度 RV 负担的 13%。从尼日利亚政府和 Gavi 的角度来看,轮状病毒疫苗接种的国家 ICER 分别为 47 美元[18;105 美元]和 62 美元[29;130 美元],每例 DALY 避免。与东南部地区 35%[24%;47%]相比,在西北部地区,轮状病毒疫苗接种预计只会将轮状病毒死亡率降低 6%[4%;9%]。基本情况 ICER 从西北部的 25 美元[10;56 美元]到南部南部的 64 美元[18;157 美元]不等。Gavi 视角的 ICER 从西北部的 33 美元[15;68 美元]到南部南部的 88 美元[35;191 美元]不等。根据单向敏感性分析,ICER 对疫苗效力最敏感,其次是估计的行政成本和轮状病毒死亡率。死亡率降低的差异主要是由于疫苗覆盖范围在区域和社会经济亚人群之间的不平等造成的。由于尼日利亚轮状病毒的负担高、持续且不平等,使用这些轮状病毒疫苗中的任何一种进行常规接种,将是减少儿童死亡率的一种具有高影响力和成本效益的策略。