Senanayake Sameera, Graves Nicholas, Healy Helen, Baboolal Keshwar, Kularatna Sanjeewa
1Australian Centre for Health Services Innovation, School of Public Health, Institute of Health and Biomedical Innovation, Queensland University of Technology, 60 Musk Ave, Kelvin Grove, Brisbane, QLD 4059 Australia.
2Royal Brisbane Hospital for Women, Brisbane, Australia.
Cost Eff Resour Alloc. 2020 May 19;18:18. doi: 10.1186/s12962-020-00213-z. eCollection 2020.
Health systems are under pressure to deliver more effective care without expansion of resources. This is particularly pertinent to diseases like chronic kidney disease (CKD) that are exacting substantial financial burden to many health systems. The aim of this study is to systematically review the Cost Utility Analysis (CUA) evidence generated across interventions for CKD patients undergoing kidney transplant (KT).
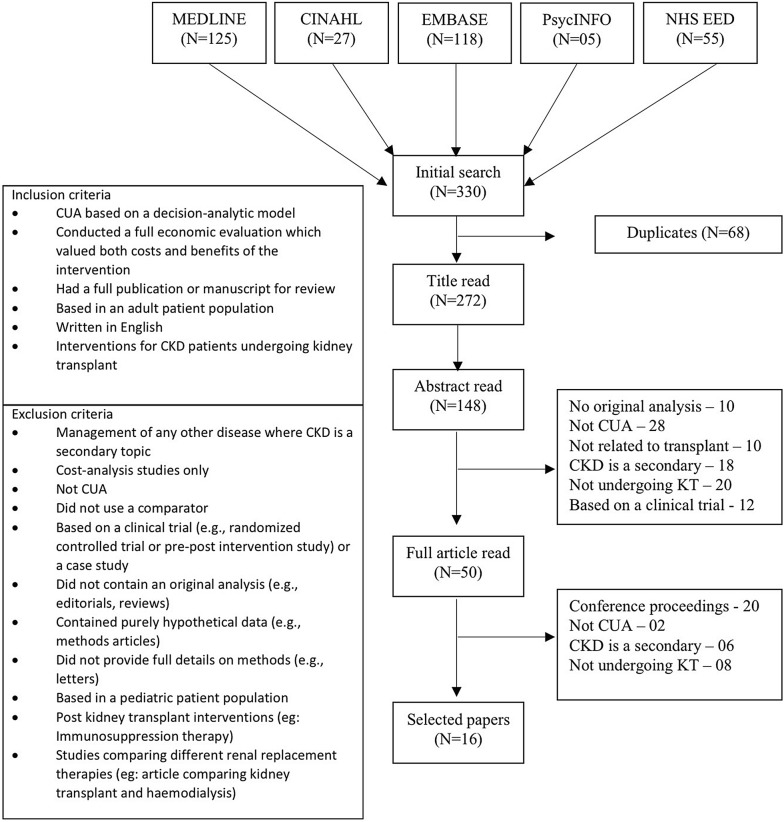
A systemic review of CUA on the interventions for CKD patients undergoing KT was carried out using a search of the MEDLINE, CINAHL, EMBASE, PsycINFO and NHS-EED. The CHEERS checklist was used as a set of good practice criteria in determining the reporting quality of the economic evaluation. Quality of the data used to inform model parameters was determined using the modified hierarchies of data sources.
A total of 330 articles identified, 16 met the inclusion criteria. Almost all (n = 15) the studies were from high income countries. Out of the 24 characteristics assessed in the CHEERS checklist, more than 80% of the selected studies reported 14 of the characteristics. Reporting of the CUA were characterized by lack of transparency of model assumptions, narrow economic perspective and incomplete assessment of the effect of uncertainty in the model parameters on the results. The data used for the economic model were satisfactory quality. The authors of 13 studies reported the intervention as cost saving and improving quality of life, whereas three studies were cost increasing and improving quality of life. In addition to the baseline analysis, sensitivity analysis was performed in all the evaluations except one. Transplanting certain high-risk donor kidneys (high risk of HIV and Hepatitis-C infected kidneys, HLA mismatched kidneys, high Kidney Donor Profile Index) and a payment to living donors, were found to be cost-effective.
The quality of economic evaluations reviewed in this paper were assessed to be satisfactory. Implementation of these strategies will significantly impact current systems of KT and require a systematic implementation plan and coordinated efforts from relevant stakeholders.
卫生系统面临着在不增加资源的情况下提供更有效护理的压力。这对于像慢性肾脏病(CKD)这样给许多卫生系统带来巨大经济负担的疾病而言尤为重要。本研究的目的是系统回顾针对接受肾移植(KT)的CKD患者的各种干预措施所产生的成本效用分析(CUA)证据。
通过检索MEDLINE、CINAHL、EMBASE、PsycINFO和NHS-EED对接受KT的CKD患者干预措施的CUA进行系统评价。在确定经济评价的报告质量时,使用CHEERS清单作为一套良好实践标准。使用修改后的数据源层次结构确定用于为模型参数提供信息的数据质量。
共识别出330篇文章,16篇符合纳入标准。几乎所有(n = 15)研究都来自高收入国家。在CHEERS清单评估的24个特征中,超过80%的入选研究报告了其中14个特征。CUA的报告特点是模型假设缺乏透明度、经济视角狭窄以及对模型参数不确定性对结果的影响评估不完整。用于经济模型的数据质量令人满意。13项研究的作者报告干预措施具有成本节约和改善生活质量的效果,而3项研究则是成本增加但改善了生活质量。除了基线分析外,除一项评估外,所有评估均进行了敏感性分析。移植某些高风险供体肾脏(艾滋病毒和丙型肝炎感染肾脏风险高、HLA不匹配肾脏、肾脏供体特征指数高)以及向活体供体支付费用被发现具有成本效益。
本文所回顾的经济评价质量被评估为令人满意。实施这些策略将对当前的KT系统产生重大影响,需要一个系统的实施计划以及相关利益攸关方的协调努力。