Morgado José P, Matias Catarina N, Reis Joana Filipa, Curto Dalia, Alves Francisco Bessone, Monteiro Cristina P
Laboratory of Physiology and Biochemistry of Exercise, Faculdade de Motricidade Humana, Universidade de Lisboa, Lisbon, Portugal.
Instituto Superior de Ciências Educativas, Lisbon, Portugal.
Front Physiol. 2020 May 12;11:471. doi: 10.3389/fphys.2020.00471. eCollection 2020.
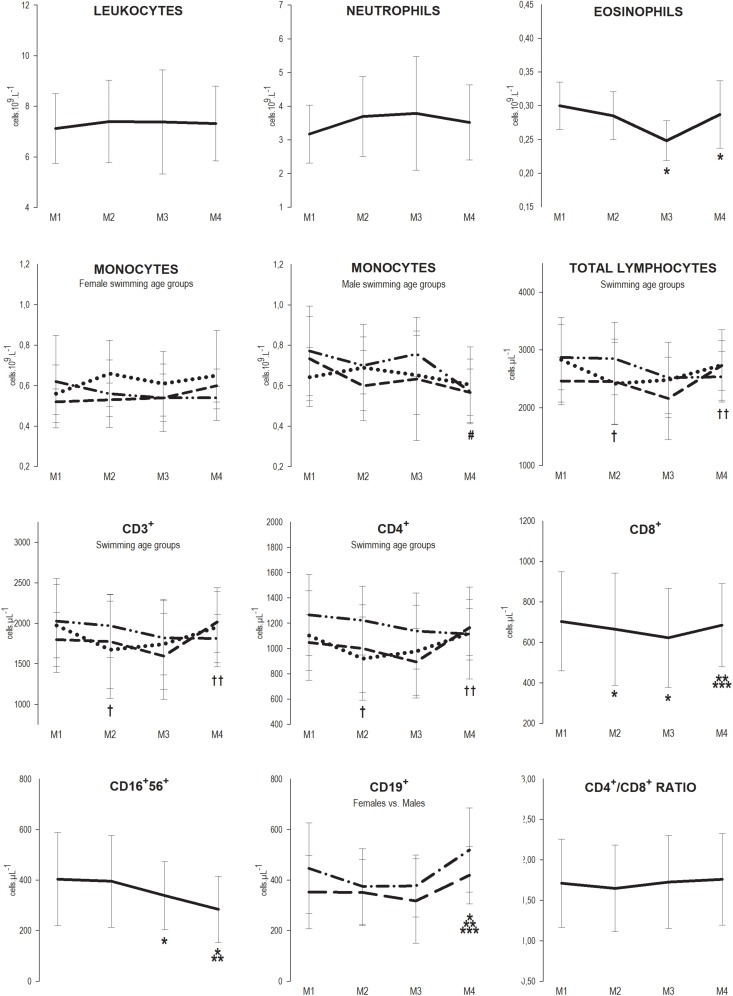
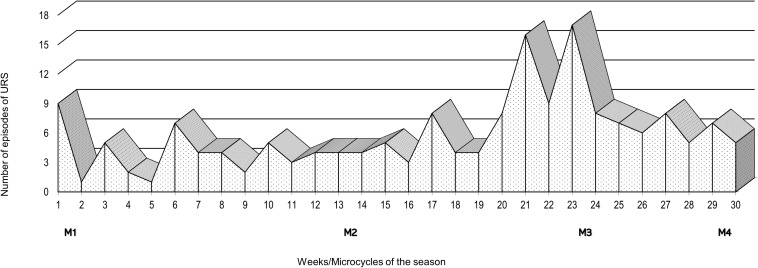
Competitive swimming requires high training load cycles including consecutive sessions with little recovery in between which may contribute to the onset of fatigue and eventually illness. We aimed to investigate immune changes over a 7-month swimming season. Fifty-four national and international level swimmers (25 females, 29 males), ranging from 13 to 20 years of age, were evaluated at rest at: M1 (beginning of the season), M2 (after the 1st macrocycle's main competition), M3 (highest training load phase of the 2nd macrocycle) and M4 (after the 2nd macrocycle's main competition) and grouped according to sex, competitive age-groups, or pubertal Tanner stages. Hemogram and the lymphocytes subsets were assessed by automatic cell counting and by flow cytometry, respectively. Self-reported Upper Respiratory Symptoms (URS) and training load were quantified. Although the values remained within the normal range reference, at M2, CD8 decreased (M1 = 703 ± 245 vs. M2 = 665 ± 278 cell μL; = 0.032) and total lymphocytes (TL, M1 = 2831 ± 734 vs. M2 = 2417 ± 714 cell μL; = 0.007), CD3 (M1 = 1974 ± 581 vs. M2 = 1672 ± 603 cell μL; = 0.003), and CD4 (M1 = 1102 ± 353 vs. M2 = 929 ± 329 cell μL; = 0.002) decreased in youth. At M3, CD8 remained below baseline (M3 = 622 ± 245 cell μL; = 0.008), eosinophils (M1 = 0.30 ± 0.04 vs. M3 = 0.25 ± 0.03 10 L; = 0.003) and CD1656 (M1 = 403 ± 184 vs. M3 = 339 ± 135 cell μL; = 0.019) decreased, and TL, CD3, and CD4 recovered in youth. At M4, CD19 were elevated (M1 = 403 ± 170 vs. M4 = 473 ± 151 cell μL; = 0.022), CD1656 continued to decrease (M4 = 284 ± 131 cell μL; < 0.001), eosinophils remained below baseline (M4 = 0.29 ± 0.05 10 L; = 0.002) and CD8 recovered; monocytes were also decreased in male seniors (M1 = 0.77 ± 0.22 vs. M4 = 0.57 ± 0.16 10 L; = 0.031). The heaviest training load and higher frequency of URS episodes happened at M3. The swimming season induced a cumulative effect toward a decrease of the number of innate immune cells, while acquired immunity appeared to be more affected at the most intense period, recovering after tapering. Younger athletes were more susceptible at the beginning of the training season than older ones.
竞技游泳需要高强度的训练周期,包括连续训练课且中间几乎没有恢复时间,这可能会导致疲劳的产生并最终引发疾病。我们旨在调查一个为期7个月的游泳赛季中的免疫变化情况。对54名年龄在13至20岁之间的国家和国际水平的游泳运动员(25名女性,29名男性)在以下时间点进行了静息状态评估:M1(赛季开始时)、M2(第一个大周期的主要比赛后)、M3(第二个大周期的最高训练负荷阶段)和M4(第二个大周期的主要比赛后),并根据性别、竞技年龄组或青春期坦纳分期进行分组。分别通过自动血细胞计数和流式细胞术评估血常规和淋巴细胞亚群。对自我报告的上呼吸道症状(URS)和训练负荷进行了量化。尽管各项数值仍在正常参考范围内,但在M2时,青年组的CD8降低(M1 = 703 ± 245对M2 = 665 ± 278细胞/μL;P = 0.032),总淋巴细胞(TL,M1 = 2831 ± 734对M2 = 2417 ± 714细胞/μL;P = 0.007)、CD3(M1 = 1974 ± 581对M2 = 1672 ± 603细胞/μL;P = 0.003)和CD4(M1 = 1102 ± 353对M = 929 ± 329细胞/μL;P = 0.002)也降低。在M3时,CD8仍低于基线水平(M3 = 622 ± 245细胞/μL;P = 0.008),嗜酸性粒细胞(M1 = 0.30 ± 0.04对M3 = 0.25 ± 0.03×10⁹/L;P = 0.003)和CD16⁺56(M1 = 403 ± 184对M3 = 339 ± 135细胞/μL;P = 0.019)降低,而青年组的TL、CD3和CD4恢复。在M4时,CD19升高(M1 = 403 ± 170对M4 = 473 ± 151细胞/μL;P = 0.022),CD16⁺56继续降低(M4 = 284 ± 131细胞/μL;P < 0.001),嗜酸性粒细胞仍低于基线水平(M4 = 0.29 ± 0.05×10⁹/L;P = 0.002)且CD8恢复;男性成年组的单核细胞也降低(M1 = 0.77 ± 0.22对M4 = 0.57 ± 0.16×10⁹/L;P = 0.031)。最大的训练负荷和URS发作的最高频率出现在M3。游泳赛季对先天免疫细胞数量的减少产生了累积效应,而获得性免疫在最激烈时期似乎受到的影响更大,在训练量减少后恢复。年轻运动员在训练赛季开始时比年长运动员更容易受到影响。