Lupa Jakob T, Raizer Jeffrey J, Helenowski Irene B, Liu Benjamin P, Kesavabhotla Kartik, Tate Matthew C
Department of Anesthesiology and Pain Medicine, University of Washington, Seattle, WA, United States.
Department of Neurology, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States.
Front Oncol. 2020 May 13;10:706. doi: 10.3389/fonc.2020.00706. eCollection 2020.
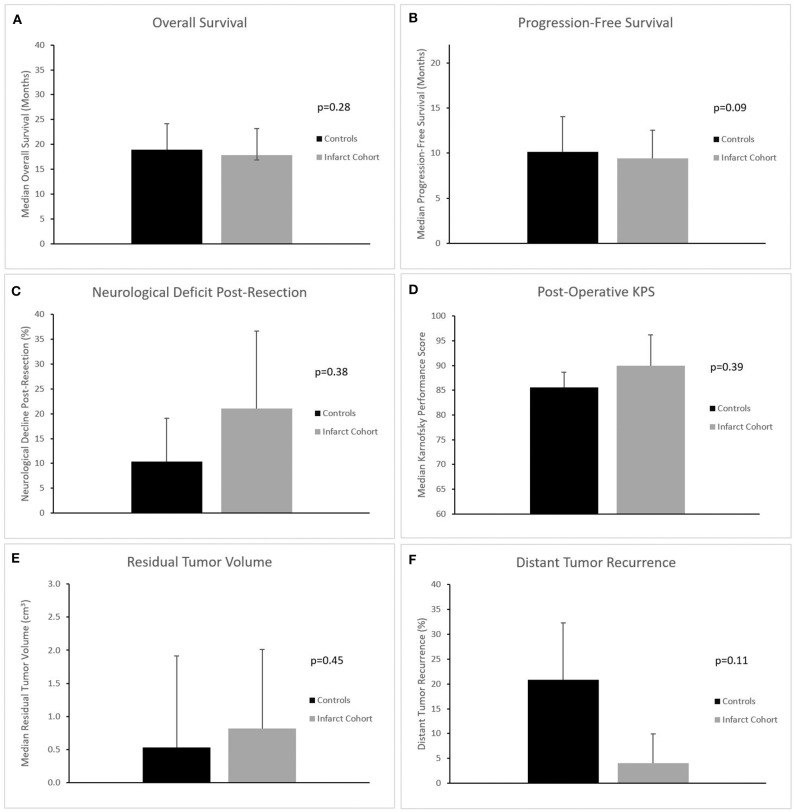
Perioperative infarcts are a known complication that can occur during the resection of glioblastoma (GBM). Recent studies suggest that gross total and even "supra-total" resections may be associated with an increased survival but the rate of complications, including perioperative ischemia, may increase with these more aggressive resection strategies. However, little is known about the impact that perioperative infarcts have on survival, functional outcomes, and tumor recurrence patterns. Our study attempted to quantify and characterize the functional consequences of a perioperative infarct, as well as risk factors associated with occurrence. Seventy-three patients with a diagnosis of GBM and perioperative ischemia by MRI were identified from the electronic medical record system. We obtained demographic, prognostic, and stroke risk factor data. Infarct volumes were calculated from diffusion-weighted MRI scans, and subjects were segregated into an infarct cohort or a control cohort based on whether the identified lesion appeared to be an infarct in an arterial distribution or instead appeared to be expected postoperative changes. A multivariate statistical analysis was performed on the dataset. Median age was 58.6 years, median post-op KPS (Karnofsky Performance Status) was 90, and median extent of resection (based on MRI) was 97.8%. Overall, perioperative arterial infarcts were uncommon (2.0%), did not have a statistically significant impact on survival (17.9 vs. 18.9 months), did not worsen neurologic function, and did not alter the pattern of recurrence. Perioperative arterial infarcts were uncommon in our patients despite aggressive resection and when present had no impact on survival or neurologic function. Given the clear benefit of maximal tumor resection, the risk of perioperative infarct should not deter maximal safe resection.
围手术期梗死是胶质母细胞瘤(GBM)切除术中已知的一种并发症。最近的研究表明,肉眼全切甚至“超全切”可能与生存期延长有关,但包括围手术期缺血在内的并发症发生率可能会随着这些更激进的切除策略而增加。然而,关于围手术期梗死对生存期、功能结局和肿瘤复发模式的影响知之甚少。我们的研究试图量化并描述围手术期梗死的功能后果以及与之相关的危险因素。通过电子病历系统识别出73例经MRI诊断为GBM且有围手术期缺血的患者。我们获取了人口统计学、预后和卒中危险因素数据。根据扩散加权MRI扫描计算梗死体积,并根据识别出的病变是呈动脉分布的梗死还是术后预期变化,将受试者分为梗死组或对照组。对数据集进行多变量统计分析。中位年龄为58.6岁,术后中位KPS(卡氏功能状态评分)为90,中位切除范围(基于MRI)为97.8%。总体而言,围手术期动脉梗死并不常见(2.0%),对生存期没有统计学上的显著影响(17.9个月对18.9个月),未使神经功能恶化,也未改变复发模式。尽管进行了激进的切除,但我们的患者围手术期动脉梗死并不常见,而且一旦出现,对生存期或神经功能没有影响。鉴于最大限度切除肿瘤有明确益处,围手术期梗死的风险不应妨碍进行最大限度的安全切除。