Cuthbert R J, Jones E, Sanjurjo-Rodríguez C, Lotfy A, Ganguly P, Churchman S M, Castana P, Tan H B, McGonagle D, Papadimitriou E, Giannoudis P V
Leeds Institute of Rheumatic and Musculoskeletal Disease, University of Leeds, Leeds LS16 7PS, UK.
Department of Biomedical Sciences, Medicine and Physiotherapy, University of A Coruña, CIBER-BBN - Institute of Biomedical Research of A Coruña (INIBIC), 15001 A Coruña, Spain.
J Clin Med. 2020 May 28;9(6):1628. doi: 10.3390/jcm9061628.
The biological mechanisms that contribute to atrophic long bone non-union are poorly understood. Multipotential mesenchymal stromal cells (MSCs) are key contributors to bone formation and are recognised as important mediators of blood vessel formation. This study examines the role of MSCs in tissue formation at the site of atrophic non-union.
Tissue and MSCs from non-union sites ( = 20) and induced periosteal (IP) membrane formed following the Masquelet bone reconstruction technique ( = 15) or bone marrow ( = 8) were compared. MSC content, differentiation, and influence on angiogenesis were measured in vitro. Cell content and vasculature measurements were performed by flow cytometry and histology, and gene expression was measured by quantitative polymerase chain reaction (qPCR).
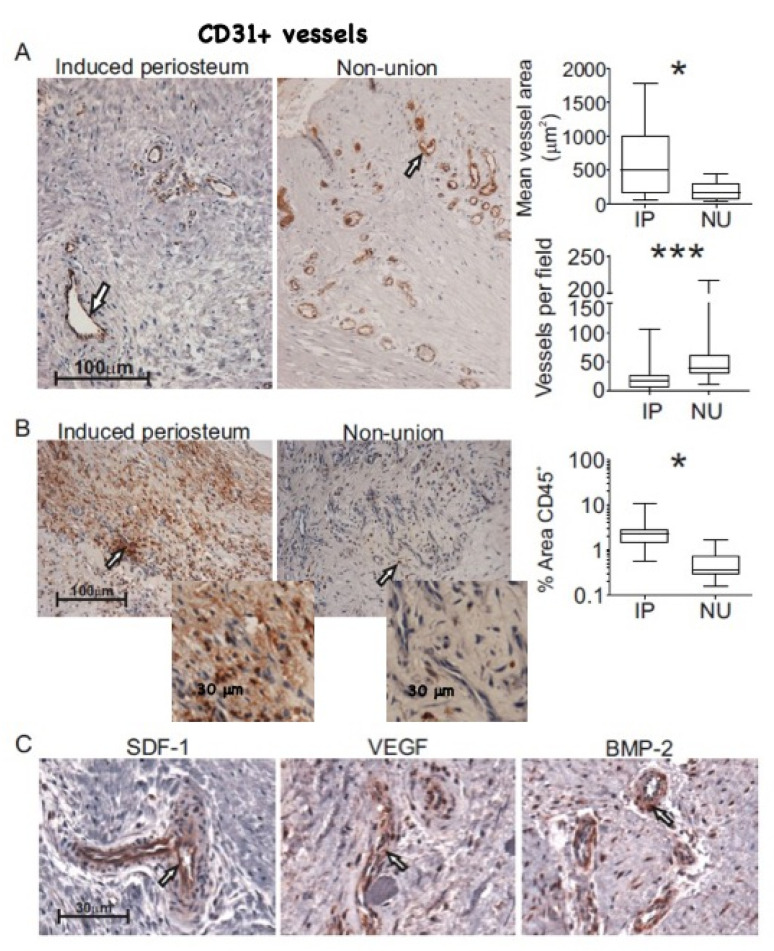
MSCs from non-union sites had comparable differentiation potential to bone marrow MSCs. Compared with induced periosteum, non-union tissue contained similar proportion of colony-forming cells, but a greater proportion of pericytes ( = 0.036), and endothelial cells ( = 0.016) and blood vessels were more numerous ( = 0.001) with smaller luminal diameter ( = 0.046). MSCs showed marked differences in angiogenic transcripts depending on the source, and those from induced periosteum, but not non-union tissue, inhibited early stages of in vitro angiogenesis.
In vitro non-union site derived MSCs have no impairment of differentiation capacity, but they differ from IP-derived MSCs in mediating angiogenesis. Local MSCs may thus be strongly implicated in the formation of the immature vascular network at the non-union site. Attention should be given to their angiogenic support profile when selecting MSCs for regenerative therapy.
导致萎缩性长骨不愈合的生物学机制尚不清楚。多能间充质基质细胞(MSCs)是骨形成的关键贡献者,被认为是血管形成的重要介质。本研究探讨了MSCs在萎缩性不愈合部位组织形成中的作用。
比较了不愈合部位(n = 20)、Masquelet骨重建技术后诱导形成的骨膜(IP)膜(n = 15)或骨髓(n = 8)的组织和MSCs。在体外测量MSCs含量、分化情况以及对血管生成的影响。通过流式细胞术和组织学进行细胞含量和脉管系统测量,并通过定量聚合酶链反应(qPCR)测量基因表达。
不愈合部位的MSCs与骨髓MSCs具有相当的分化潜能。与诱导骨膜相比,不愈合组织中集落形成细胞的比例相似,但周细胞比例更高(P = 0.036),内皮细胞比例更高(P = 0.016),血管数量更多(P = 0.001),管腔直径更小(P = 0.046)。根据来源不同,MSCs在血管生成转录本上表现出显著差异,来自诱导骨膜而非不愈合组织的MSCs抑制体外血管生成的早期阶段。
体外从不愈合部位获取的MSCs分化能力无损害,但在介导血管生成方面与来自IP的MSCs不同。因此,局部MSCs可能与不愈合部位不成熟血管网络的形成密切相关。在选择用于再生治疗的MSCs时,应关注其血管生成支持特征。