Matheson Center for Health Care Studies, The University of Utah, Salt Lake City.
Health Services Research and Administration, University of Nebraska Medical Center, Omaha.
JAMA Netw Open. 2020 Jun 1;3(6):e206745. doi: 10.1001/jamanetworkopen.2020.6745.
Overdose from opioids causes nearly 50 000 deaths in the US each year. Adverse consequences from opioid use are particularly pronounced among low-income and publicly insured individuals. However, little is known about patterns of opioid prescribing among non-US-born individuals in the US.
To examine the association of opioid prescriptions with non-US-born status, particularly among patients clinically diagnosed with pain.
DESIGN, SETTING, AND PARTICIPANTS: This cross-sectional analysis assessed opioid prescriptions among US-born and non-US-born adults using the 2016-2017 Medical Expenditure Panel Survey. Data were analyzed from January 1, 2016, to December 31, 2017.
Practitioner-verified binary variable for any opioid prescription, number of prescriptions received, and a count variable for number of days of prescribed medicine. Multivariable logistic and negative binomial regression adjusted for sex, age, race/ethnicity, marital status, educational level, poverty, insurance status, clinical diagnoses for acute or chronic pain, census region, and survey year.
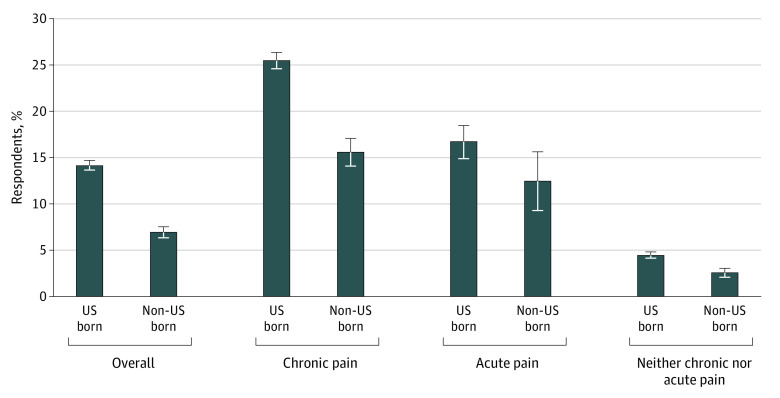
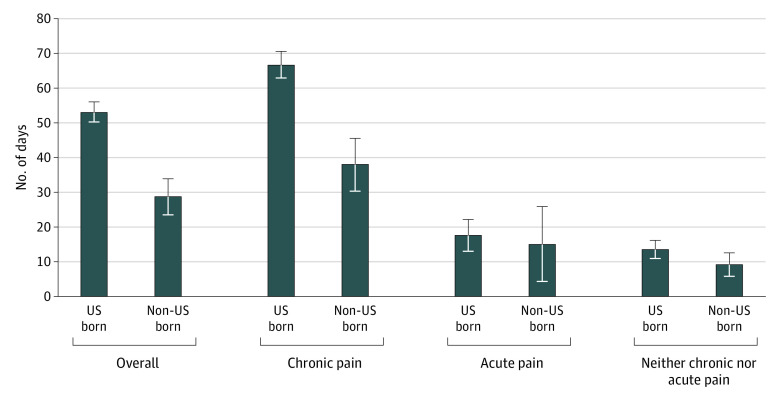
Among all 48 162 respondents (mean [SD] age, 47.0 [18.1] years; 25 831 [53.6%] female), 14.2% of US-born and 7.0% of non-US-born individuals received at least 1 opioid prescription within a 12-month period. For those diagnosed with chronic pain, 25.5% of US-born individuals and 15.6% of non-US-born individuals received at least 1 opioid prescription within a 12-month period. In multivariable logistic regression, non-US-born individuals had 35% lower odds of receiving an opioid prescription than US-born individuals (adjusted odds ratio, 0.65; 95% CI, 0.56-0.74). In negative binomial regression adjusting for confounding factors, non-US-born individuals with chronic pain who were prescribed opioids received significantly fewer days' supply (50.0; 95% CI, 40.0-59.9) than US-born individuals (77.2; 95% CI, 72.7-81.6). Differences between US-born and non-US-born individuals were not statistically significant for patients with acute pain (16.7% [95% CI, 14.9%-18.4%] of US-born individuals received opioids vs 12.5% [95% CI, 9.3%-15.6%] of non-US-born individuals). Non-US-born individuals with less than 5 years of residency in the US were significantly less likely to receive a prescription for opioids than were those with longer residency after adjustment for type of pain and other confounding factors (adjusted odds ratio, 0.51; 95% CI, 0.30-0.88).
The findings suggest that non-US-born individuals, particularly those with shorter US residency, are less likely to be prescribed opioids than US-born individuals.
在美国,每年有近 5 万人因阿片类药物过量而死亡。在低收入和公共保险人群中,阿片类药物使用的不良后果尤为明显。然而,人们对非美国出生的人在美国的阿片类药物处方模式知之甚少。
研究阿片类药物处方与非美国出生身份之间的关系,特别是在临床上诊断为疼痛的患者中。
设计、设置和参与者:本横断面分析使用 2016-2017 年医疗支出面板调查评估了美国出生和非美国出生成年人的阿片类药物处方。数据于 2016 年 1 月 1 日至 2017 年 12 月 31 日进行分析。
执业医师验证的二进制变量,用于任何阿片类药物处方、接受的处方数量和规定药物天数的计数变量。多变量逻辑回归和负二项回归调整了性别、年龄、种族/民族、婚姻状况、教育程度、贫困、保险状况、急性或慢性疼痛的临床诊断、人口普查区域和调查年份。
在所有 48162 名受访者(平均[SD]年龄 47.0[18.1]岁;25831[53.6%]女性)中,14.2%的美国出生者和 7.0%的非美国出生者在 12 个月内至少接受过 1 次阿片类药物处方。对于被诊断为慢性疼痛的患者,25.5%的美国出生者和 15.6%的非美国出生者在 12 个月内至少接受过 1 次阿片类药物处方。在多变量逻辑回归中,非美国出生者接受阿片类药物处方的可能性比美国出生者低 35%(调整后的优势比,0.65;95%CI,0.56-0.74)。在调整混杂因素的负二项回归中,接受阿片类药物处方的慢性疼痛非美国出生者的用药天数明显减少(50.0;95%CI,40.0-59.9),而美国出生者为 77.2;95%CI,72.7-81.6)。对于急性疼痛患者,美国出生者和非美国出生者之间的差异无统计学意义(16.7%[95%CI,14.9%-18.4%]的美国出生者接受阿片类药物治疗,而 12.5%[95%CI,9.3%-15.6%]的非美国出生者)。在美国居住不到 5 年的非美国出生者与居住时间较长者相比,接受阿片类药物处方的可能性显著降低,调整疼痛类型和其他混杂因素后(调整后的优势比,0.51;95%CI,0.30-0.88)。
研究结果表明,非美国出生者,特别是在美国居住时间较短者,接受阿片类药物处方的可能性低于美国出生者。