Bertoluci Marcello Casaccia, Salles João Eduardo Nunes, Silva-Nunes José, Pedrosa Hermelinda Cordeiro, Moreira Rodrigo Oliveira, da Silva Duarte Rui Manuel Calado, da Costa Carvalho Davide Mauricio, Trujilho Fábio Rogério, Dos Santos Raposo João Filipe Cancela, Parente Erika Bezerra, Valente Fernando, de Moura Fábio Ferreira, Hohl Alexandre, Melo Miguel, Araujo Francisco Garcia Pestana, de Araújo Principe Rosa Maria Monteiro Castro, Kupfer Rosane, Costa E Forti Adriana, Valerio Cynthia Melissa, Ferreira Hélder José, Duarte João Manuel Sequeira, Saraiva José Francisco Kerr, Rodacki Melanie, Castelo Maria Helane Costa Gurgel, Monteiro Mariana Pereira, Branco Patrícia Quadros, de Matos Pedro Manuel Patricio, de Melo Pereira de Magalhães Pedro Carneiro, Betti Roberto Tadeu Barcellos, Réa Rosângela Roginski, Trujilho Thaisa Dourado Guedes, Pinto Lana Catani Ferreira, Leitão Cristiane Bauermann
Internal Medicine Department, School of Medicine, Universidade Federal do Rio Grande do Sul (UFRGS), Rua Ramiro Barcelos, 2350, 4º Andar, Porto Alegre, RS 90035-007 Brazil.
Endocrinology Unit, Hospital de Clínicas de Porto Alegre (HCPA-UFRGS), Rua Ramiro Barcelos, 2350, 4º Andar, Porto Alegre, RS 90035-007 Brazil.
Diabetol Metab Syndr. 2020 May 24;12:45. doi: 10.1186/s13098-020-00551-1. eCollection 2020.
In current management of type 2 diabetes (T2DM), cardiovascular and renal prevention have become important targets to be achieved. In this context, a joint panel of four endocrinology societies from Brazil and Portugal was established to develop an evidence-based guideline for treatment of hyperglycemia in T2DM.
MEDLINE (via PubMed) was searched for randomized clinical trials, meta-analyses, and observational studies related to diabetes treatment. When there was insufficient high-quality evidence, expert opinion was sought. Updated positions on treatment of T2DM patients with heart failure (HF), atherosclerotic CV disease (ASCVD), chronic kidney disease (CKD), and patients with no vascular complications were developed. The degree of recommendation and the level of evidence were determined using predefined criteria.
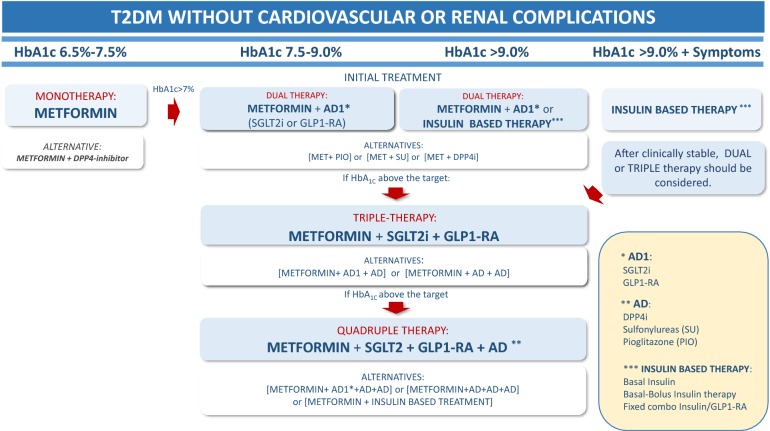
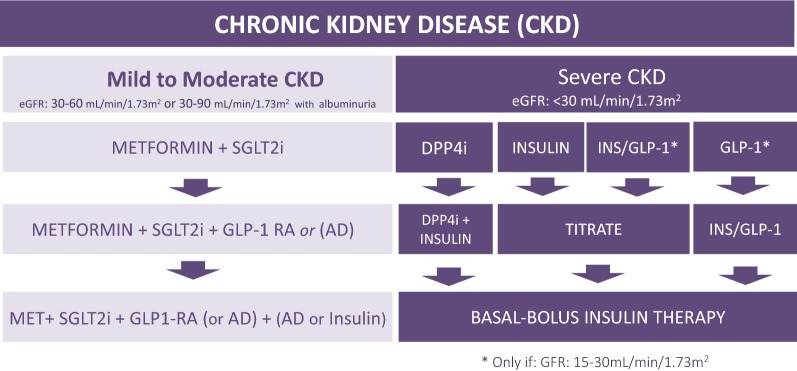
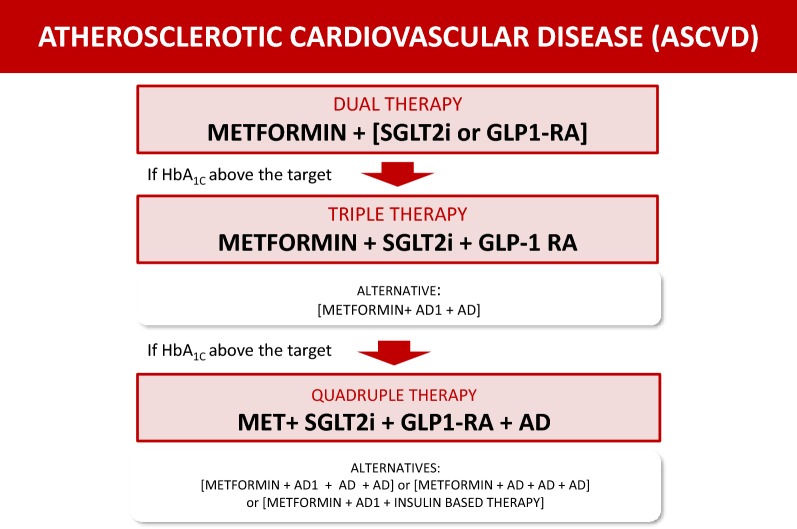
In non-pregnant adults, the recommended HbA target is below 7%. Higher levels are recommended in frail older adults and patients at higher risk of hypoglycemia. Lifestyle modification is recommended at all phases of treatment. Metformin is the first choice when HbA is 6.5-7.5%. When HbA is 7.5-9.0%, dual therapy with metformin plus an SGLT2i and/or GLP-RA (first-line antidiabetic agents, AD1) is recommended due to cardiovascular and renal benefits. If an AD1 is unaffordable, other antidiabetic drugs (AD) may be used. Triple or quadruple therapy should be considered when HbA remains above target. In patients with clinical or subclinical atherosclerosis, the combination of one AD1 plus metformin is the recommended first-line therapy to reduce cardiovascular events and improve blood glucose control. In stable heart failure with low ejection fraction (< 40%) and glomerular filtration rate (eGFR) > 30 mL/min/1.73 m, metformin plus an SGLT-2i is recommended to reduce cardiovascular mortality and heart failure hospitalizations and improve blood glucose control. In patients with diabetes-associated chronic kidney disease (CKD) (eGFR 30-60 mL/min/1.73 m or eGFR 30-90 mL/min/1.73 m with albuminuria > 30 mg/g), the combination of metformin and an SGLT2i is recommended to attenuate loss of renal function, reduce albuminuria and improve blood glucose control. In patients with severe renal failure, insulin-based therapy is recommended to improve blood glucose control. Alternatively, GLP-RA, DPP4i, gliclazide MR and pioglitazone may be considered to reduce albuminuria. In conclusion, the current evidence supports individualizing anti-hyperglycemic treatment for T2DM.
在2型糖尿病(T2DM)的当前管理中,心血管和肾脏预防已成为重要的治疗目标。在此背景下,巴西和葡萄牙的四个内分泌学会联合成立了一个小组,以制定基于证据的T2DM高血糖治疗指南。
通过MEDLINE(经由PubMed)检索与糖尿病治疗相关的随机临床试验、荟萃分析和观察性研究。当高质量证据不足时,征求专家意见。制定了关于心力衰竭(HF)、动脉粥样硬化性心血管疾病(ASCVD)、慢性肾脏病(CKD)的T2DM患者以及无血管并发症患者治疗的最新立场。使用预定义标准确定推荐程度和证据水平。
在非妊娠成年人中,推荐的糖化血红蛋白(HbA)目标低于7%。对于身体虚弱的老年人和低血糖风险较高的患者,建议设定更高的目标值。在治疗的各个阶段均建议进行生活方式调整。当HbA为6.5 - 7.5%时,二甲双胍是首选药物。当HbA为7.5 - 9.0%时,由于具有心血管和肾脏益处,建议二甲双胍联合钠 - 葡萄糖协同转运蛋白2抑制剂(SGLT2i)和/或胰高血糖素样肽 - 1受体激动剂(GLP - RA,一线抗糖尿病药物,AD1)进行双重治疗。如果AD1无法承受,则可使用其他抗糖尿病药物(AD)。当HbA仍高于目标值时,应考虑三联或四联治疗。对于有临床或亚临床动脉粥样硬化的患者,推荐AD1联合二甲双胍作为一线治疗,以减少心血管事件并改善血糖控制。对于射血分数低(<40%)且肾小球滤过率(eGFR)>30 mL/min/1.73m²的稳定心力衰竭患者,建议使用二甲双胍联合SGLT - 2i,以降低心血管死亡率和心力衰竭住院率,并改善血糖控制。对于糖尿病相关慢性肾脏病(CKD)患者(eGFR为30 - 60 mL/min/1.73m²或eGFR为30 - 90 mL/min/1.73m²且白蛋白尿>30mg/g),建议二甲双胍联合SGLT2i,以减轻肾功能丧失、减少白蛋白尿并改善血糖控制。对于严重肾衰竭患者,建议采用胰岛素治疗以改善血糖控制。另外,可考虑使用GLP - RA、二肽基肽酶4抑制剂(DPP4i)、格列齐特缓释片和吡格列酮来减少白蛋白尿。总之,当前证据支持对T2DM进行个体化降糖治疗。