Sharma Esseim, McCauley Brian, Ghosalkar Dhairyasheel S, Atalay Michael, Collins Scott, Parulkar Anshul, Sheikh Wasiq, Ahmed Malik B, Chu Antony
Department of Cardiology, The Warren Alpert Medical School of Brown University, Providence, RI, USA.
Department of Cardiology, Rhode Island Hospital, Providence, RI, USA.
Cardiol Res. 2020 Jun;11(3):155-167. doi: 10.14740/cr1011. Epub 2020 May 3.
Atrioventricular block requiring permanent pacemaker (PPM) implantation is a common complication of transcatheter aortic valve replacement (TAVR). The mechanism of atrioventricular (AV) block during TAVR is not fully understood, but it may be due to the mechanical stress of TAVR deployment, resulting in possible injury to the nearby compact AV node. Aortic valve calcification (AVC) may worsen this condition and has been associated with an increased risk for post-TAVR PPM implantation. We performed a retrospective analysis to determine if AVC is predictive for long-term right ventricular (RV) pacing in post-TAVR pacemaker patients at 30 days.
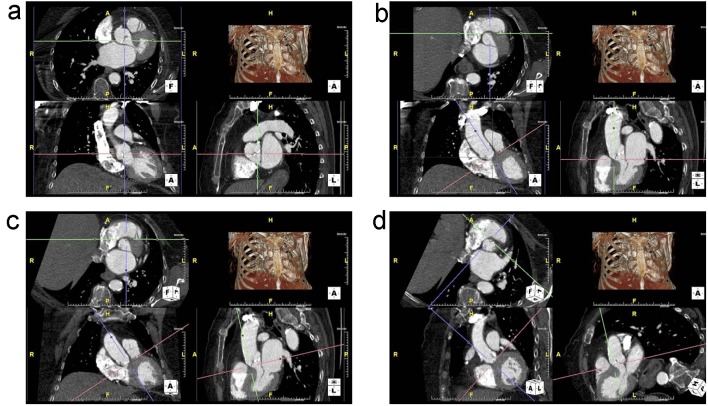
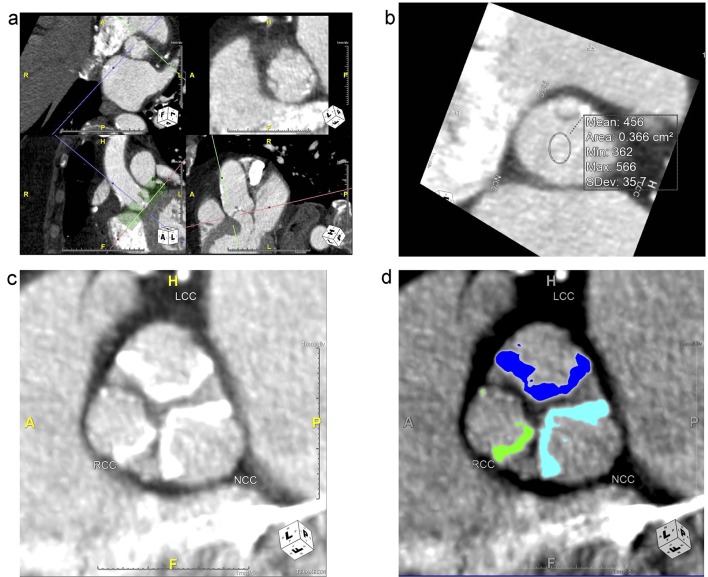
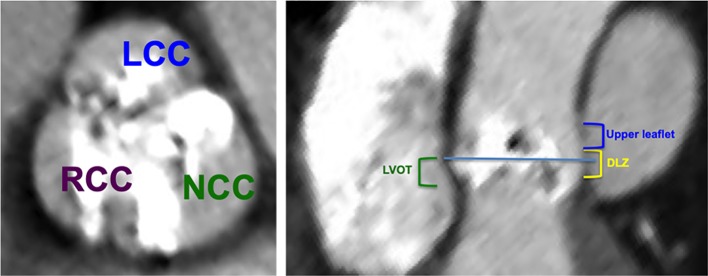
A total of 262 consecutive patients who underwent TAVR with a balloon-expandable valve were analyzed. AVC data were derived from contrast-enhanced computed tomography and characterized by leaflet sector and region.
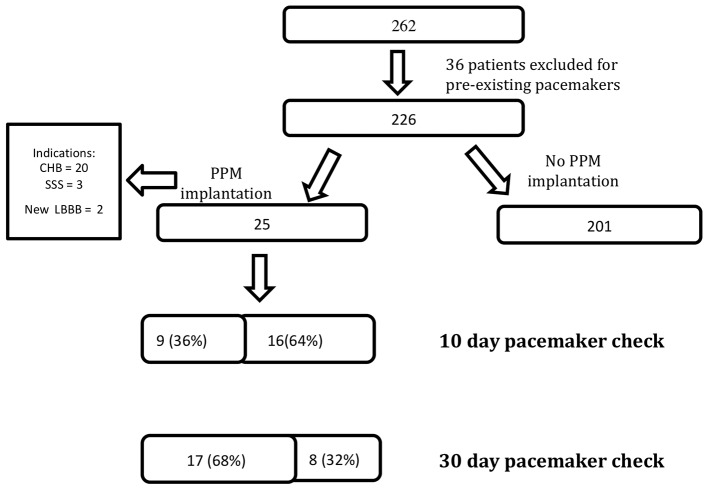
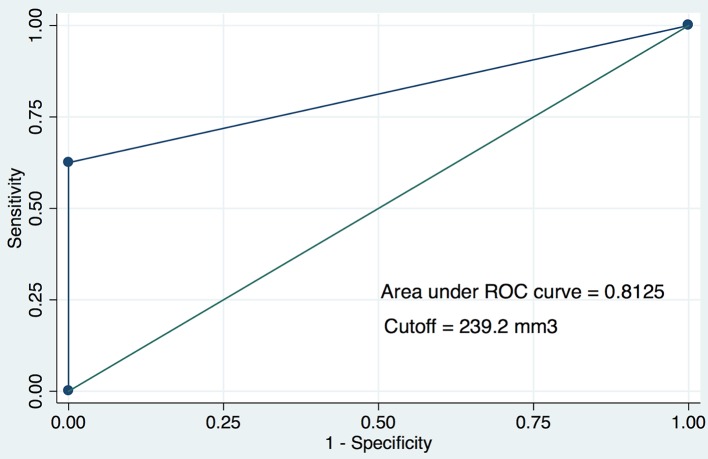
A total of 25 patients (11.1%) required post-TAVR PPM implantation. Seventeen patients did not require RV pacing at 30 days. Nine of these 17 patients had no RV pacing requirement within 10 days. The presence of intra-procedural heart block (P = 0.004) was the only significant difference between patients who did not require PPM and those who required PPM but they were not RV pacing-dependent at 30 days. Non-coronary cusp (NCC) calcium volume was significantly higher in patients who were pacemaker-dependent at 30 days (P = 0.01) and a calcium volume of > 239.2 mm in the NCC was strongly predictive of pacemaker dependence at 30 days (area under the curve (AUC) = 0.813). Pre-existing right bundle branch block (RBBB) (odds ratio (OR) 105.4, P = 0.004), bifascicular block (OR 12.5, P = 0.02), QRS duration (OR 70.43, P = 0.007) and intra-procedural complete heart block (OR 12.83, P = 0.03) were also predictive of pacemaker dependence at 30 days.
In patients who required PPM after TAVR, quantification of AVC by non-coronary leaflet calcium volume was found to be a novel predictor for RV pacing dependence at 30 days. The association of NCC calcification and PPM dependence may be related to the proximity of the conduction bundle to the non-coronary leaflet. Further studies are necessary to improve risk prediction for long-term RV pacing requirements following TAVR.
需要植入永久起搏器(PPM)的房室传导阻滞是经导管主动脉瓣置换术(TAVR)的常见并发症。TAVR 期间房室(AV)传导阻滞的机制尚未完全明确,但可能是由于 TAVR 植入时的机械应力,导致附近致密房室结可能受损。主动脉瓣钙化(AVC)可能会使这种情况恶化,并与 TAVR 后植入 PPM 的风险增加有关。我们进行了一项回顾性分析,以确定 AVC 是否可预测 TAVR 后起搏器植入患者 30 天时的长期右心室(RV)起搏情况。
对 262 例连续接受球囊扩张瓣膜 TAVR 的患者进行分析。AVC 数据来自对比增强计算机断层扫描,并按瓣叶扇形区域进行特征描述。
共有 25 例患者(11.1%)需要在 TAVR 后植入 PPM。17 例患者在 30 天时不需要 RV 起搏。这 17 例患者中有 9 例在 10 天内不需要 RV 起搏。术中发生心脏传导阻滞(P = 0.004)是不需要 PPM 的患者与需要 PPM 但在 30 天时不依赖 RV 起搏的患者之间唯一的显著差异。30 天时依赖起搏器的患者非冠状动脉瓣叶(NCC)钙体积显著更高(P = 0.01),NCC 中钙体积>239.2 mm 强烈预测 30 天时的起搏器依赖(曲线下面积(AUC)= 0.813)。既往存在右束支传导阻滞(RBBB)(比值比(OR)105.4,P = 0.004)、双分支传导阻滞(OR 12.5,P = 0.02)、QRS 时限(OR 70.4³,P = 0.007)和术中完全性心脏传导阻滞(OR 12.8³,P = 0.03)也可预测 30 天时的起搏器依赖。
在 TAVR 后需要 PPM 的患者中,通过非冠状动脉瓣叶钙体积对 AVC 进行量化被发现是 30 天时 RV 起搏依赖的一种新的预测指标。NCC 钙化与 PPM 依赖的关联可能与传导束靠近非冠状动脉瓣叶有关。需要进一步研究以改善 TAVR 后长期 RV 起搏需求的风险预测。