Department of Clinical Sciences Lund, Neurology, Skåne University Hospital, Lund University, Getingevägen 4, 222 41, Lund, Sweden.
Department of Clinical Sciences Lund, Clinical Neurophysiology, Skane University Hospital, Lund University, Lund, Sweden.
Intensive Care Med. 2020 Oct;46(10):1852-1862. doi: 10.1007/s00134-020-06080-9. Epub 2020 Jun 3.
To assess the performance of a 4-step algorithm for neurological prognostication after cardiac arrest recommended by the European Resuscitation Council (ERC) and the European Society of Intensive Care Medicine (ESICM).
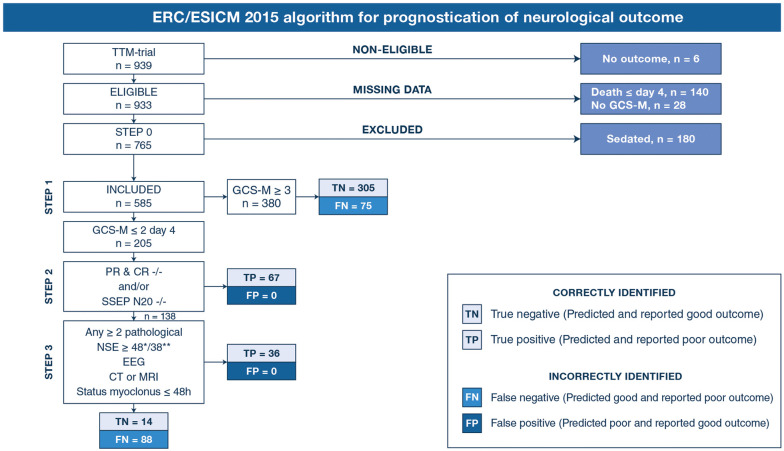
Retrospective descriptive analysis with data from the Target Temperature Management (TTM) Trial. Associations between predicted and actual neurological outcome were investigated for each step of the algorithm with results from clinical neurological examinations, neuroradiology (CT or MRI), neurophysiology (EEG and SSEP) and serum neuron-specific enolase. Patients examined with Glasgow Coma Scale Motor Score (GCS-M) on day 4 (72-96 h) post-arrest and available 6-month outcome were included. Poor outcome was defined as Cerebral Performance Category 3-5. Variations of the ERC/ESICM algorithm were explored within the same cohort.
The ERC/ESICM algorithm identified poor outcome patients with 38.7% sensitivity (95% CI 33.1-44.7) and 100% specificity (95% CI 98.8-100) in a cohort of 585 patients. An alternative cut-off for serum neuron-specific enolase, an alternative EEG-classification and variations of the GCS-M had minor effects on the sensitivity without causing false positive predictions. The highest overall sensitivity, 42.5% (95% CI 36.7-48.5), was achieved when prognosticating patients irrespective of GCS-M score, with 100% specificity (95% CI 98.8-100) remaining.
The ERC/ESICM algorithm and all exploratory multimodal variations thereof investigated in this study predicted poor outcome without false positive predictions and with sensitivities 34.6-42.5%. Our results should be validated prospectively, preferably in patients where withdrawal of life-sustaining therapy is uncommon to exclude any confounding from self-fulfilling prophecies.
评估欧洲复苏委员会(ERC)和欧洲危重病医学会(ESICM)推荐的用于心脏骤停后神经预后的 4 步算法的性能。
回顾性描述性分析,数据来自目标温度管理(TTM)试验。使用临床神经检查、神经影像学(CT 或 MRI)、神经生理学(EEG 和 SSEP)和血清神经元特异性烯醇化酶的结果,对算法的每一步骤进行预测和实际神经结果之间的关联进行研究。包括在心脏骤停后第 4 天(72-96 小时)接受格拉斯哥昏迷量表运动评分(GCS-M)检查且可获得 6 个月结局的患者。预后不良定义为脑功能预后分类 3-5 级。在同一队列中探索了 ERC/ESICM 算法的变化。
在 585 例患者的队列中,ERC/ESICM 算法以 38.7%的敏感性(95%CI 33.1-44.7)和 100%的特异性(95%CI 98.8-100)识别预后不良的患者。神经元特异性烯醇化酶的替代截断值、替代 EEG 分类和 GCS-M 的变化对敏感性影响较小,而不会导致假阳性预测。当不考虑 GCS-M 评分对所有患者进行预后预测时,敏感性最高,为 42.5%(95%CI 36.7-48.5),特异性仍为 100%(95%CI 98.8-100)。
本研究中调查的 ERC/ESICM 算法及其所有探索性多模态变化均能预测预后不良,且无假阳性预测,敏感性为 34.6-42.5%。我们的结果应前瞻性验证,最好在很少有患者停止生命支持治疗的情况下进行,以排除自我实现预言的任何混杂。