Department of Neurology, Mayo Clinic, Rochester, MN.
Department of Health Sciences Research, Mayo Clinic, Rochester, MN.
Mayo Clin Proc. 2020 Jun;95(6):1195-1205. doi: 10.1016/j.mayocp.2020.01.028.
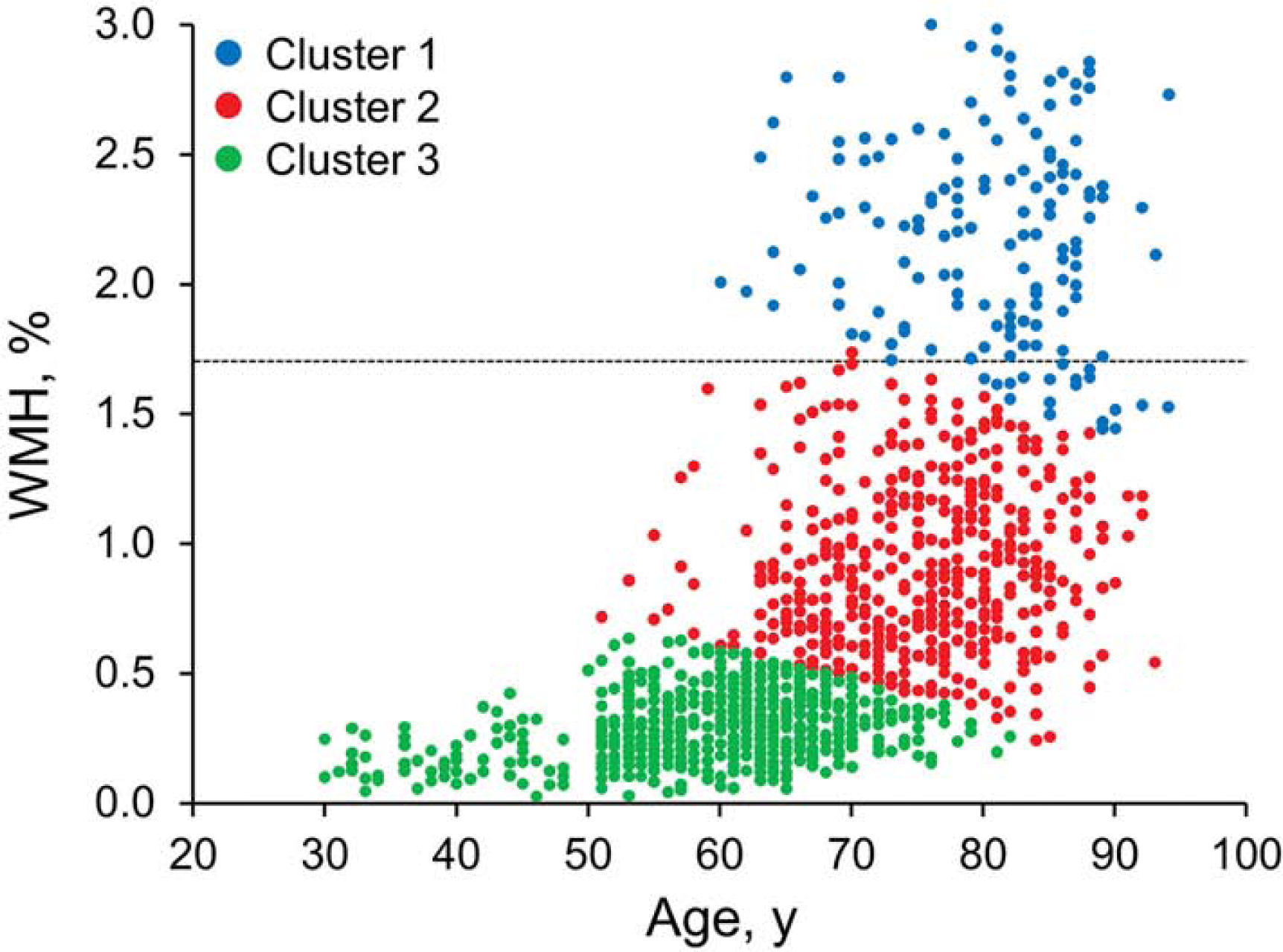
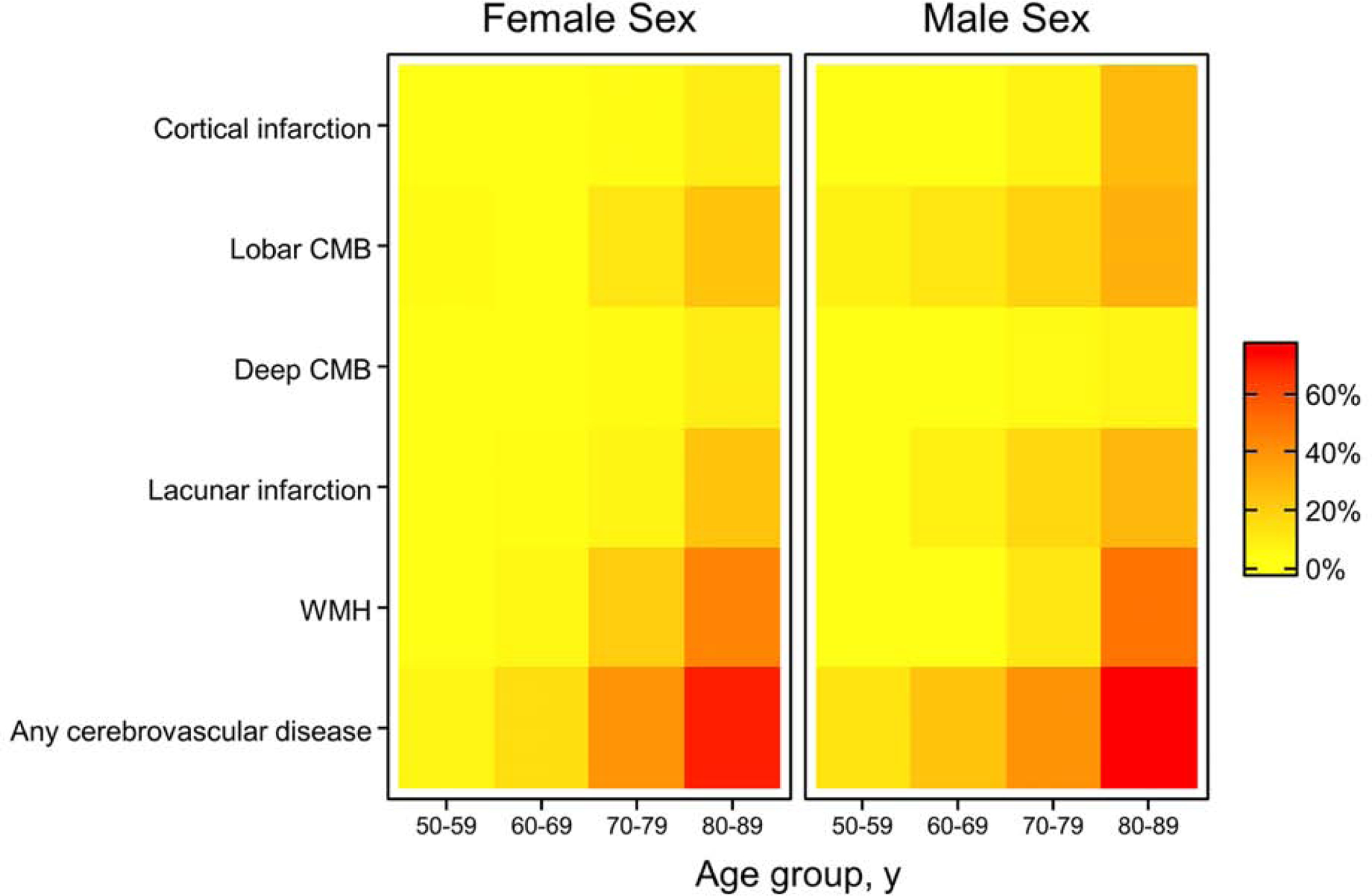
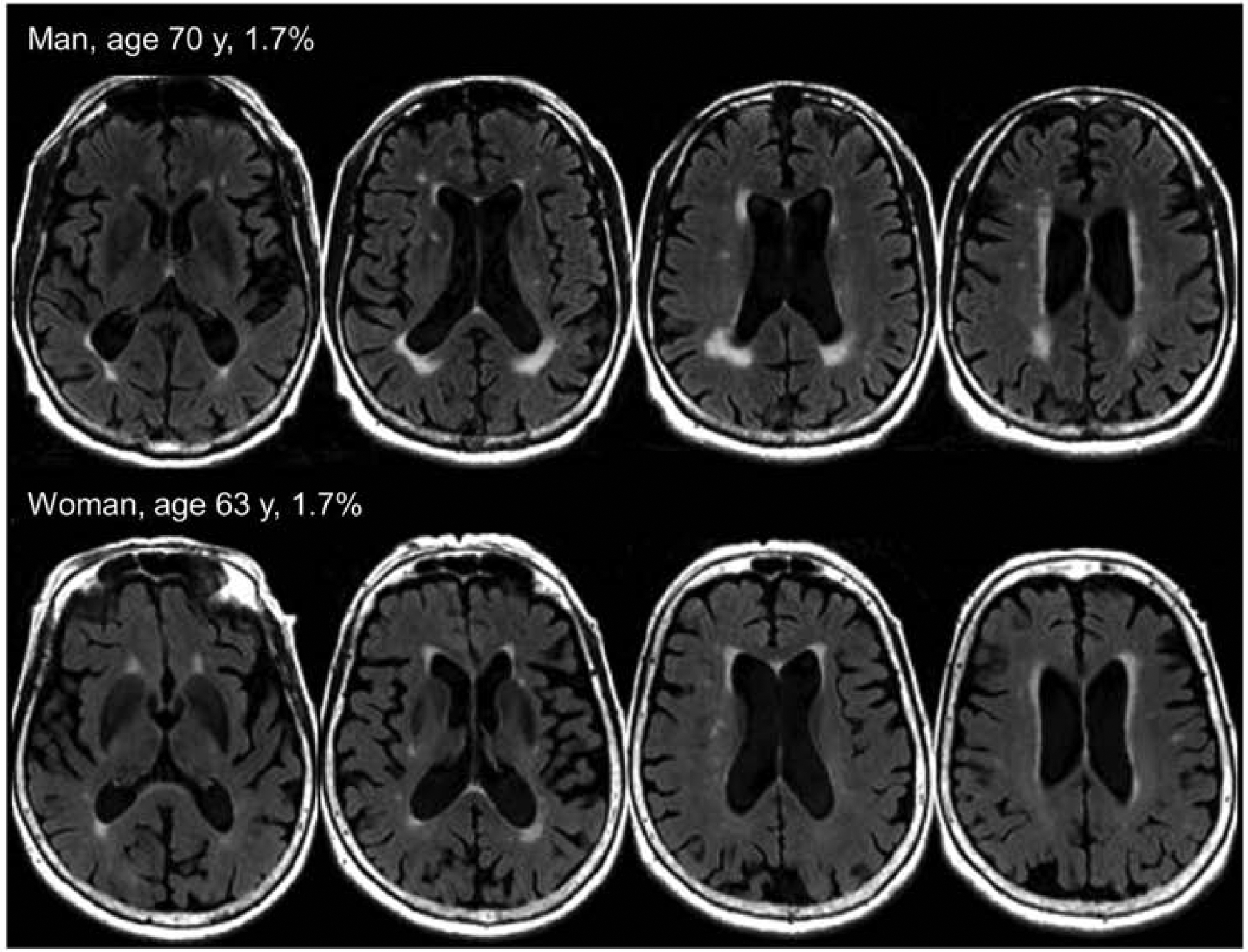
To report population age-specific prevalence of core cerebrovascular disease lesions (infarctions, cerebral microbleeds, and white-matter hyperintensities detected with magnetic resonance imaging); estimate cut points for white-matter hyperintensity positivity; investigate sex differences in prevalence; and estimate prevalence of any core cerebrovascular disease features.
Participants in the population-based Mayo Clinic Study of Aging aged 50 to 89 years underwent fluid-attenuated inversion recovery and T2* gradient-recalled echo magnetic resonance imaging to assess cerebrovascular disease between October 10, 2011, and September 29, 2017. We characterized each participant as having infarct, normal versus abnormal white-matter hyperintensity, cerebral microbleed, or a combination of lesions. Prevalence of cerebrovascular disease biomarkers was derived through adjustment for nonparticipation and standardization to the population of Olmsted County, Minnesota.
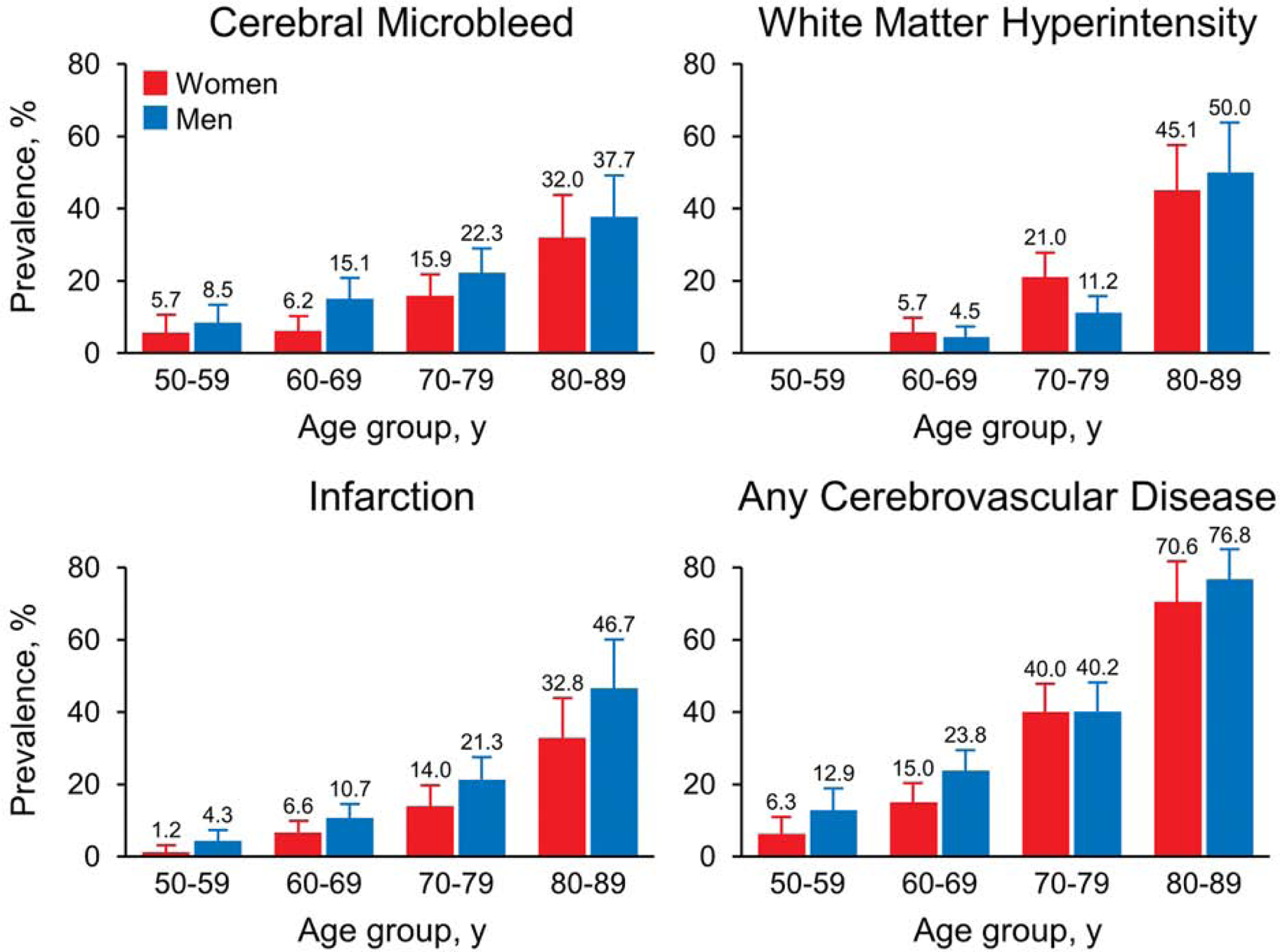
Among 1462 participants without dementia (median [range] age, 68 [50 to 89] y; men, 52.7%), core cerebrovascular disease features increased with age. Prevalence (95% CI) of cerebral microbleeds was 13.6% (11.6%-15.6%); infarcts, 11.7% (9.7%-13.8%); and abnormal white-matter hyperintensity, 10.7% (8.7%-12.6%). Infarcts and cerebral microbleeds were more common among men. In contrast, abnormal white-matter hyperintensity was more common among women ages 60 to 79 y and men, ages 80 y and older. Prevalence of any core cerebrovascular disease feature determined by presence of at least one cerebrovascular disease feature increased from 9.5% (ages 50 to 59 y) to 73.8% (ages 80 to 89 y).
Whereas this study focused on participants without dementia, the high prevalence of cerebrovascular disease imaging lesions in elderly persons makes assignment of clinical relevance to cognition and other downstream manifestations more probabilistic than deterministic.
报告人群特定年龄的核心脑血管疾病病变(通过磁共振成像检测到的梗死、脑微出血和脑白质高信号)的流行率;估计脑白质高信号阳性的切点;研究性别在流行率方面的差异;并估计任何核心脑血管疾病特征的流行率。
2011 年 10 月 10 日至 2017 年 9 月 29 日,在明尼苏达州奥姆斯特德县 Mayo 诊所研究老龄化的人群基础研究中,年龄在 50 至 89 岁的参与者接受了液体衰减反转恢复和 T2*梯度回波磁共振成像,以评估脑血管疾病。我们将每个参与者描述为存在梗死、正常或异常脑白质高信号、脑微出血或病变的组合。脑血管疾病生物标志物的流行率是通过对未参与研究的人员进行调整和将其标准化到明尼苏达州奥姆斯特德县人群中得出的。
在 1462 名无痴呆症(中位[范围]年龄,68[50 至 89]岁;男性占 52.7%)参与者中,核心脑血管疾病特征随年龄增长而增加。脑微出血的流行率(95%CI)为 13.6%(11.6%至 15.6%);梗死为 11.7%(9.7%至 13.8%);异常脑白质高信号为 10.7%(8.7%至 12.6%)。男性中梗死和脑微出血更为常见。相比之下,在 60 至 79 岁的女性和 80 岁及以上的男性中,异常脑白质高信号更为常见。任何核心脑血管疾病特征的流行率(通过至少存在一种脑血管疾病特征确定)从 9.5%(50 至 59 岁)增加到 73.8%(80 至 89 岁)。
尽管本研究重点关注无痴呆症的参与者,但老年人脑血管疾病影像学病变的高流行率使得将认知和其他下游表现的临床相关性归因于概率而不是确定性更为重要。