Department of Psychiatry, University of Rochester, Rochester, NY, United States of America.
Department of Internal Medicine, Kaiser Permanente Santa Clara, Santa Clara, CA, United States of America.
PLoS One. 2020 Jun 5;15(6):e0233996. doi: 10.1371/journal.pone.0233996. eCollection 2020.
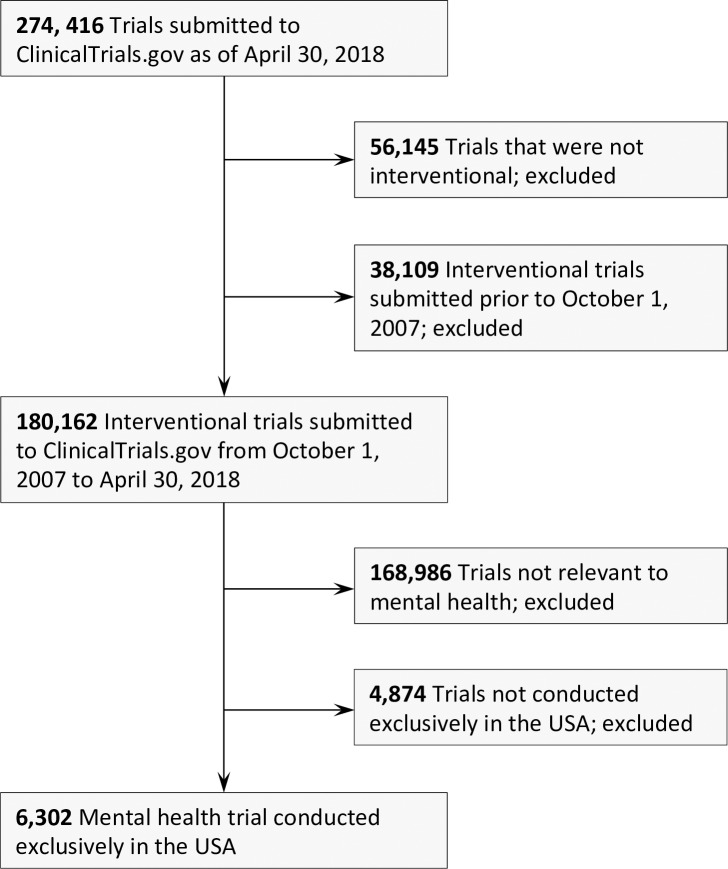
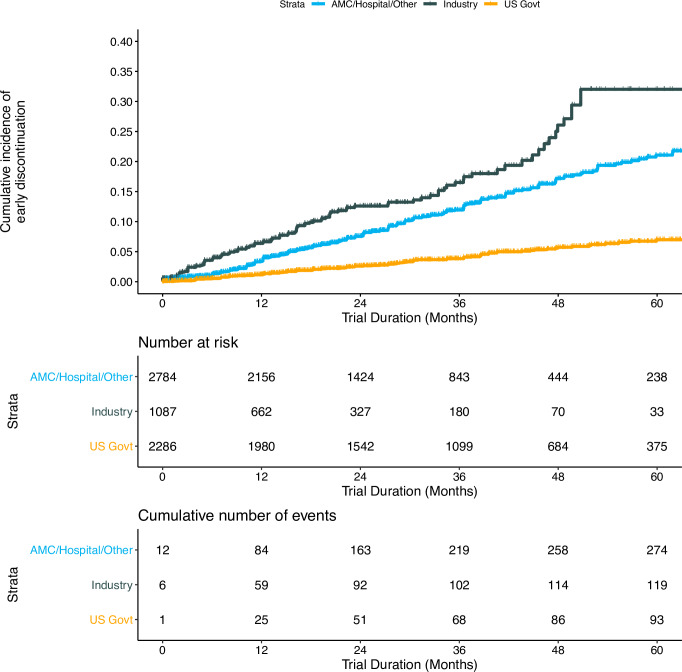
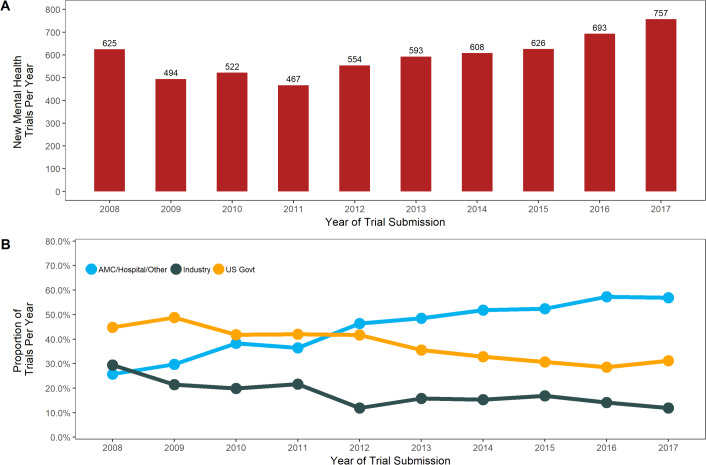
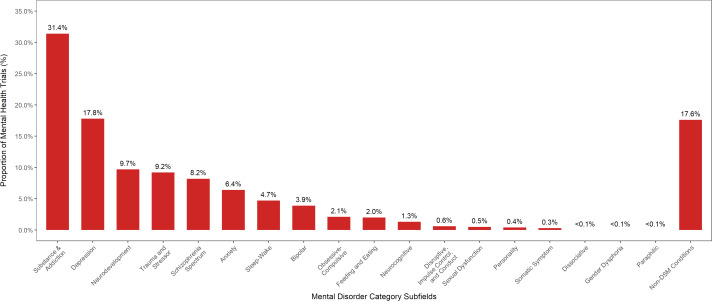
While the epidemiologic burden of mental health disorders in the United States has been well described over the past decade, we know relatively little about trends in how these disorders are being studied through clinical research. We examined all US interventional mental health trials submitted to ClinicalTrials.gov between October 1, 2007 and April 30, 2018 to identify trends in trial characteristics, comparisons with non-mental health trials, and trial attributes associated with discontinuation and results reporting. International data were excluded to minimize potential confounding. Over this period, mental health and non-mental health trials grew at similar rates, though Industry and US government-funded trials declined and academic medical center/hospital/other (AMC/Hosp/Oth) funded trials grew faster in mental health research. The proportion of trials with safeguards against bias, including blinding and oversight by data monitoring committees (DMCs), decreased. This occurred during growth in the proportion of trials studying behavioral and non-pharmacological interventions, which often cannot be blinded and do not require DMC oversight. There was concurrent decline in pharmaceutical trials. There was significant growth in trials studying Non-DSM (Diagnostic and Statistical Manual-5) conditions (e.g. suicidality and wellness), as well as substance use, anxiety, and neurocognitive disorders. One in 12 trials was discontinued. Trial discontinuation was associated with industry and AMC/Hosp/Oth funders, pharmaceutical interventions, and lack of DMC oversight. Only 29.9% of completed trials reported results to the registry. Decreased results reporting was associated with behavioral interventions, phase 1 trials, and industry and AMC/Hosp/Oth funders. The main implications of these data are that funding is shifting away from traditional government and industry sources, there is increasing interest in non-pharmacological treatments and Non-DSM conditions, and there are changing norms in trial design characteristics regarding safeguards against bias. These trends can guide researchers and funding bodies when considering the trajectory of future mental health research.
尽管过去十年已经很好地描述了美国精神健康障碍的流行病学负担,但我们对这些障碍在临床研究中是如何研究的趋势知之甚少。我们研究了 2007 年 10 月 1 日至 2018 年 4 月 30 日期间提交给 ClinicalTrials.gov 的所有美国干预性精神健康试验,以确定试验特征、与非精神健康试验的比较以及与试验中止和结果报告相关的试验属性的趋势。排除国际数据是为了最大限度地减少潜在的混杂因素。在此期间,精神健康和非精神健康试验的增长率相似,尽管工业界和美国政府资助的试验减少,而学术医学中心/医院/其他(AMC/Hosp/Oth)资助的试验在精神健康研究中增长更快。防止偏见的试验比例(包括盲法和数据监测委员会(DMC)监督)下降。这是在研究行为和非药物干预的试验比例增加的同时发生的,这些试验往往无法进行盲法并且不需要 DMC 监督。制药试验也同时减少。研究非 DSM(诊断和统计手册-5)疾病(例如自杀和健康)以及物质使用、焦虑和神经认知障碍的试验显著增加。每 12 个试验中就有一个中止。试验中止与工业界和 AMC/Hosp/Oth 资助者、制药干预以及缺乏 DMC 监督有关。只有 29.9%的完成试验向注册处报告了结果。结果报告减少与行为干预、1 期试验以及工业界和 AMC/Hosp/Oth 资助者有关。这些数据的主要含义是,资金正在从传统的政府和工业来源转移,人们对非药物治疗和非 DSM 疾病越来越感兴趣,以及关于防止偏见的试验设计特征的规范正在发生变化。这些趋势可以为研究人员和资助机构提供指导,以考虑未来精神健康研究的轨迹。