Minici Roberto, Paone Sara, Talarico Marisa, Zappia Lorenzo, Abdalla Karim, Petullà Maria, Laganà Domenico
Radiology Division, Department of Experimental and Clinical Medicine, Magna Graecia University of Catanzaro, University Hospital Mater Domini, Viale Europa, 88100, Catanzaro, CZ, Italy.
IRC - FSH, Department of Health Sciences, Magna Graecia University of Catanzaro, Catanzaro, Italy.
CVIR Endovasc. 2020 Jun 8;3(1):29. doi: 10.1186/s42155-020-00120-7.
The spread of percutaneous arterial catheterization in diagnostic and therapeutic procedures has led to a parallel increase of vascular access site complications. The incidence of these events is between 0.2-1%. A detailed analysis of injuries by type of procedure shows a higher incidence of injuries after therapeutic procedures (3%) than those observed for diagnostic ones (1%), due to the greater size of the vascular devices used and the necessity to frequently administer anticoagulant and antiplatelet therapy during procedures. The iatrogenic arterial injuries requiring treatment are the pseudoaneurysm, arteriovenous fistula, arterial rupture and dissection. Less frequent complications include distal embolization of the limbs, nerve damage, abscess and lymphocele. Moreover, the use of percutaneous vascular closure devices (VCD) has further expanded the types of complications, with an increased risk of stenosis, thrombosis, distal embolism and infection. Our work aims to bring the personal 10 years' experience in the percutaneous treatment of vascular access-site complications.
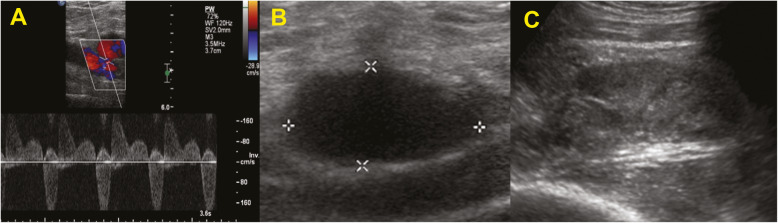
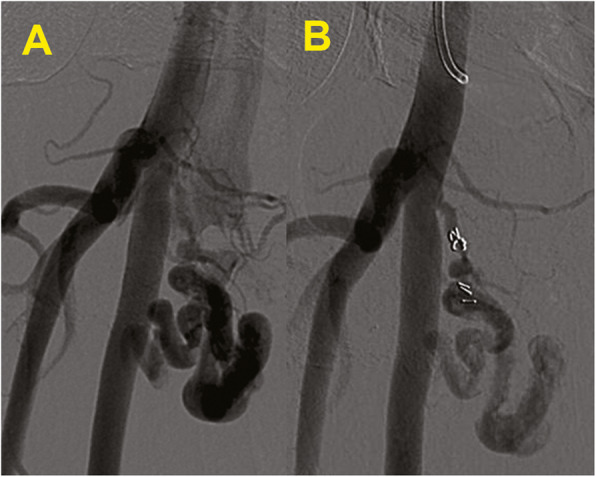
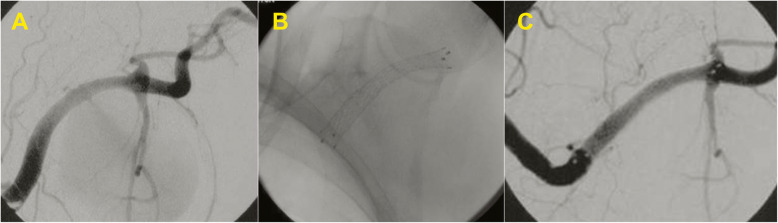
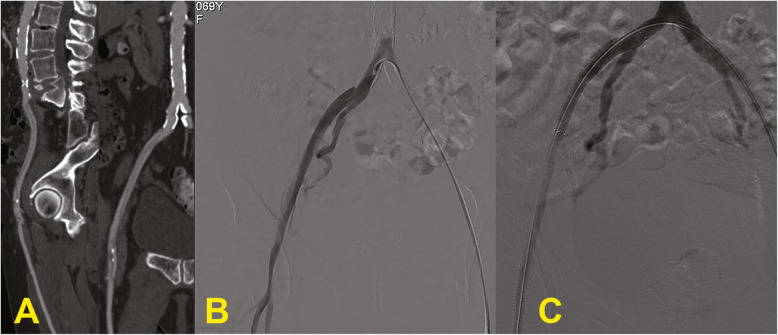
Ninety-two pseudoaneurysms (PSA), 12 arteriovenous fistulas (AVF), 15 retrograde dissections (RD) and 11 retroperitoneal bleedings (RB) have been selected and treated. In 120/130 cases there were no periprocedural complications with immediate technical success (92.3%). Nine femoral PSA, treated with percutaneous ultrasound-guided thrombin injection, showed a failure to close the sac and therefore they were treated by PTA balloon inflation with a contralateral approach and cross-over technique. Only one case of brachial dissection, in which the prolonged inflation of the balloon has not led to a full reimbursement of the dissection flap, was then surgically repaired. At the 7 days follow-up, complications were two abscesses in retroperitoneal bleedings, treated by percutaneous drainage. At 3 months, acute occlusion of 3 covered femoral stents occurred, then treated by loco-regional thrombolysis and PTA. A total of 18 major complications was recorded at 2 years, with a complication rate at 2 years of 13.8%.
The percutaneous treatment of vascular access-site complications is the first-choice treatment. It represents a safe and effective option, validated by a high technical success rate and a low long-term complication rate, that allows avoiding the surgical approach in most cases.
经皮动脉导管插入术在诊断和治疗程序中的广泛应用导致血管穿刺部位并发症相应增加。这些事件的发生率在0.2%至1%之间。按手术类型对损伤进行的详细分析表明,由于所用血管装置尺寸更大以及手术过程中频繁使用抗凝和抗血小板治疗的必要性,治疗性手术后的损伤发生率(3%)高于诊断性手术(1%)。需要治疗的医源性动脉损伤包括假性动脉瘤、动静脉瘘、动脉破裂和夹层。较少见的并发症包括肢体远端栓塞、神经损伤、脓肿和淋巴囊肿。此外,经皮血管闭合装置(VCD)的使用进一步扩大了并发症的类型,增加了狭窄、血栓形成、远端栓塞和感染的风险。我们的工作旨在分享经皮治疗血管穿刺部位并发症的10年个人经验。
共选择并治疗了92例假性动脉瘤(PSA)、12例动静脉瘘(AVF)、15例逆行夹层(RD)和11例腹膜后出血(RB)。130例中有120例在围手术期无并发症,手术即刻成功(92.3%)。9例股部PSA采用经皮超声引导下注射凝血酶治疗,结果显示囊袋未闭合,因此采用对侧入路和交叉技术通过球囊扩张血管成形术(PTA)进行治疗。仅1例肱动脉夹层,球囊长时间扩张未使夹层瓣完全复位,随后进行了手术修复。在7天随访时,腹膜后出血出现2例脓肿,经皮引流治疗。在3个月时,3个带膜股动脉支架发生急性闭塞,随后采用局部溶栓和PTA治疗。2年时共记录到18例严重并发症,2年并发症发生率为13.8%。
经皮治疗血管穿刺部位并发症是首选治疗方法。它是一种安全有效的选择,技术成功率高且长期并发症率低,在大多数情况下可避免手术治疗。