Nguyen Long H, Drew David A, Joshi Amit D, Guo Chuan-Guo, Ma Wenjie, Mehta Raaj S, Sikavi Daniel R, Lo Chun-Han, Kwon Sohee, Song Mingyang, Mucci Lorelei A, Stampfer Meir J, Willett Walter C, Eliassen A Heather, Hart Jaime E, Chavarro Jorge E, Rich-Edwards Janet W, Davies Richard, Capdevila Joan, Lee Karla A, Lochlainn Mary Ni, Varsavsky Thomas, Graham Mark S, Sudre Carole H, Cardoso M Jorge, Wolf Jonathan, Ourselin Sebastien, Steves Claire J, Spector Tim D, Chan Andrew T
Division of Gastroenterology, Massachusetts General Hospital and Harvard Medical School. Boston, MA, USA.
Clinical and Translational Epidemiology Unit, Massachusetts General Hospital and Harvard Medical School. Boston, MA, USA.
medRxiv. 2020 May 25:2020.04.29.20084111. doi: 10.1101/2020.04.29.20084111.
Data for frontline healthcare workers (HCWs) and risk of SARS-CoV-2 infection are limited and whether personal protective equipment (PPE) mitigates this risk is unknown. We evaluated risk for COVID-19 among frontline HCWs compared to the general community and the influence of PPE.
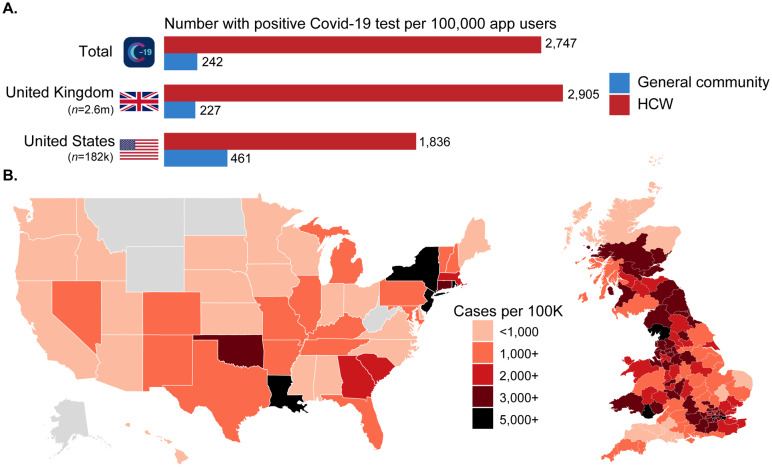
We performed a prospective cohort study of the general community, including frontline HCWs, who reported information through the COVID Symptom Study smartphone application beginning on March 24 (United Kingdom, U.K.) and March 29 (United States, U.S.) through April 23, 2020. We used Cox proportional hazards modeling to estimate multivariate-adjusted hazard ratios (aHRs) of a positive COVID-19 test.
Among 2,035,395 community individuals and 99,795 frontline HCWs, we documented 5,545 incident reports of a positive COVID-19 test over 34,435,272 person-days. Compared with the general community, frontline HCWs had an aHR of 11·6 (95% CI: 10·9 to 12·3) for reporting a positive test. The corresponding aHR was 3·40 (95% CI: 3·37 to 3·43) using an inverse probability weighted Cox model adjusting for the likelihood of receiving a test. A symptom-based classifier of predicted COVID-19 yielded similar risk estimates. Compared with HCWs reporting adequate PPE, the aHRs for reporting a positive test were 1·46 (95% CI: 1·21 to 1·76) for those reporting PPE reuse and 1·31 (95% CI: 1·10 to 1·56) for reporting inadequate PPE. Compared with HCWs reporting adequate PPE who did not care for COVID-19 patients, HCWs caring for patients with documented COVID-19 had aHRs for a positive test of 4·83 (95% CI: 3·99 to 5·85) if they had adequate PPE, 5·06 (95% CI: 3·90 to 6·57) for reused PPE, and 5·91 (95% CI: 4·53 to 7·71) for inadequate PPE.
Frontline HCWs had a significantly increased risk of COVID-19 infection, highest among HCWs who reused PPE or had inadequate access to PPE. However, adequate supplies of PPE did not completely mitigate high-risk exposures.
Zoe Global Ltd., Wellcome Trust, EPSRC, NIHR, UK Research and Innovation, Alzheimer's Society, NIH, NIOSH, Massachusetts Consortium on Pathogen Readiness.
一线医护人员感染新冠病毒(SARS-CoV-2)的数据有限,个人防护装备(PPE)能否降低这种风险尚不清楚。我们评估了一线医护人员与普通社区人群相比感染新冠病毒的风险以及个人防护装备的影响。
我们对普通社区人群(包括一线医护人员)进行了一项前瞻性队列研究,这些人群从3月24日(英国)和3月29日(美国)开始至2020年4月23日通过“新冠症状研究”智能手机应用程序报告信息。我们使用Cox比例风险模型来估计新冠病毒检测呈阳性的多变量调整风险比(aHRs)。
在2,035,395名社区个体和99,795名一线医护人员中,在34,435,272人日期间,我们记录了5,545例新冠病毒检测呈阳性的事件报告。与普通社区相比,一线医护人员报告检测呈阳性的aHR为11.6(95%置信区间:10.9至12.3)。使用逆概率加权Cox模型对接受检测的可能性进行调整后,相应的aHR为3.40(95%置信区间:3.37至3.43)。基于症状的新冠病毒预测分类器得出了类似的风险估计值。与报告个人防护装备充足的医护人员相比,报告重复使用个人防护装备的医护人员报告检测呈阳性的aHR为1.46(95%置信区间:1.21至1.76),报告个人防护装备不足的aHR为1.31(95%置信区间:1.10至1.56)。与报告个人防护装备充足且不护理新冠患者的医护人员相比,护理确诊新冠患者的医护人员若个人防护装备充足,报告检测呈阳性的aHR为4.83(95%置信区间:3.99至5.85);若重复使用个人防护装备,aHR为5.06(95%置信区间:3.90至6.57);若个人防护装备不足,aHR为5.91(95%置信区间:4.53至7.71)。
一线医护人员感染新冠病毒的风险显著增加,在重复使用个人防护装备或个人防护装备供应不足的医护人员中风险最高。然而,充足的个人防护装备供应并不能完全降低高风险暴露。
佐伊全球有限公司、惠康信托基金会、工程和物理科学研究委员会、英国国家卫生研究院、英国研究与创新署、阿尔茨海默病协会、美国国立卫生研究院、美国国家职业安全与健康研究所、马萨诸塞州病原体准备联盟。