EPIUnit - Institute of Public Health, University of Porto, Porto, Portugal.
Department of Mathematics and Applications, University of Minho, Campus de Gualtar, 4710-057, Braga, Portugal.
Sci Rep. 2020 Jun 12;10(1):9535. doi: 10.1038/s41598-020-65201-y.
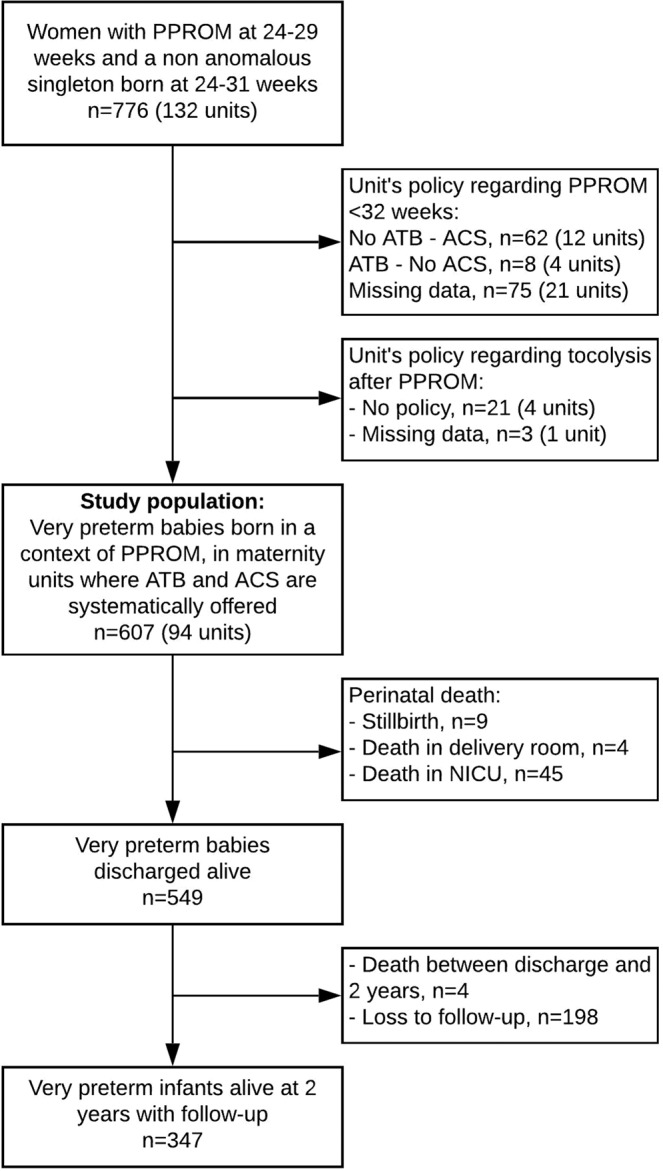
After preterm premature rupture of membranes (PPROM), antibiotics and antenatal steroids are effective evidence-based interventions, but the use of tocolysis is controversial. We investigated whether a unit policy of tocolysis use after PPROM is associated with prolonged gestation and improved outcomes for very preterm infants in units that systematically use these other evidence-based treatments. From the prospective, observational, population-based EPICE cohort study (all very preterm births in 19 regions from 11 European countries, 2011-2012), we included 607 women with a singleton pregnancy and PPROM at 24-29 weeks' gestation, of whom 101, 195 and 311 were respectively managed in 17, 32 and 45 units with no-use, restricted and liberal tocolysis policies for PPROM. The association between unit policies and outcomes (early-onset sepsis, survival at discharge, survival at discharge without severe morbidity and survival at two years without gross motor impairment) was investigated using three-level random-intercept logistic regression models, showing no differences in neonatal or two-year outcomes by unit policy. Moreover, there was no association between unit policies and prolongation of gestation in a multilevel survival analysis. Compared to a unit policy of no-use of tocolysis after PPROM, a liberal or restricted policy is not associated with improved obstetric, neonatal or two-year outcomes.
胎膜早破(PPROM)后,抗生素和产前类固醇是有效的循证干预措施,但抑制宫缩的使用存在争议。我们研究了在系统使用这些其他循证治疗方法的单位中,PPROM 后使用抑制宫缩的单位政策是否与延长胎龄和改善极早产儿的结局相关。这项研究来自前瞻性、观察性、基于人群的 EPICE 队列研究(11 个欧洲国家的 19 个地区所有极早产儿,2011-2012 年),共纳入了 607 名单胎妊娠和 24-29 周胎膜早破的孕妇,其中 17、32 和 45 个单位分别采取了不使用、限制和自由使用抑制宫缩的 PPROM 单位政策,分别有 101、195 和 311 名孕妇。采用三级随机截距逻辑回归模型研究单位政策与结局(早发性败血症、出院时存活率、出院时无严重发病率存活率和两年时无粗大运动障碍存活率)之间的关系,结果显示不同单位政策对新生儿或两年结局无差异。此外,在多水平生存分析中,单位政策与胎龄延长之间也没有关联。与不使用抑制宫缩的单位政策相比,自由或限制使用抑制宫缩的单位政策与改善产科、新生儿或两年结局无关。