Weiss Salome, Sen Indrani, Huang Ying, Harmsen W Scott, Bower Thomas C, Oderich Gustavo S, Goodney Philip P, DeMartino Randall R
Division of Vascular and Endovascular Surgery, Mayo Clinic, Rochester, MN; Department of Cardiovascular Surgery, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland.
Division of Vascular and Endovascular Surgery, Mayo Clinic, Rochester, MN.
Ann Vasc Surg. 2020 Nov;69:62-73. doi: 10.1016/j.avsg.2020.06.004. Epub 2020 Jun 17.
The aim of the study was to analyze aortic-related outcomes after diagnosis of aortic dissection (AD), intramural hematoma (IMH), and penetrating aortic ulcer (PAU) from a population-based approach.
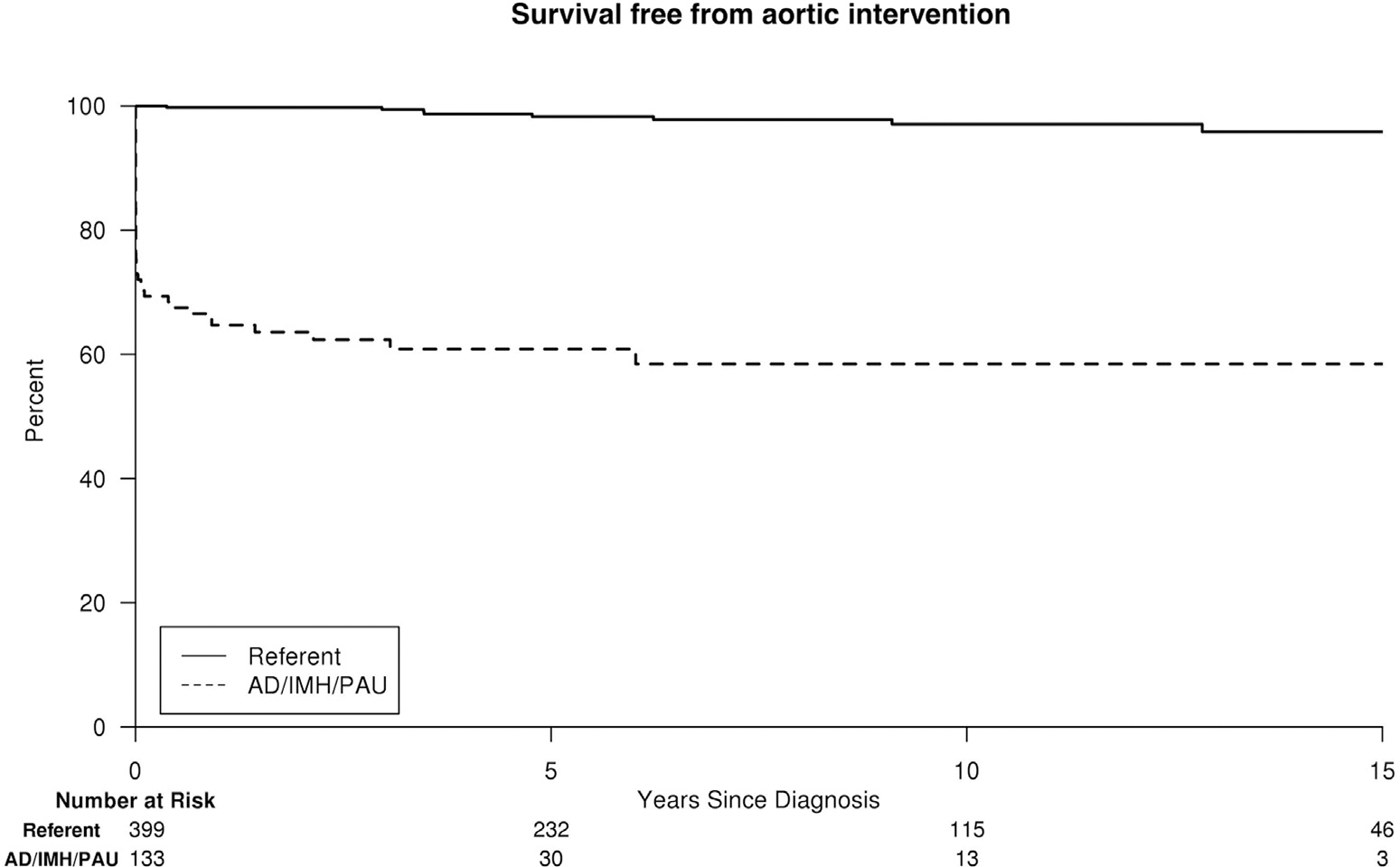
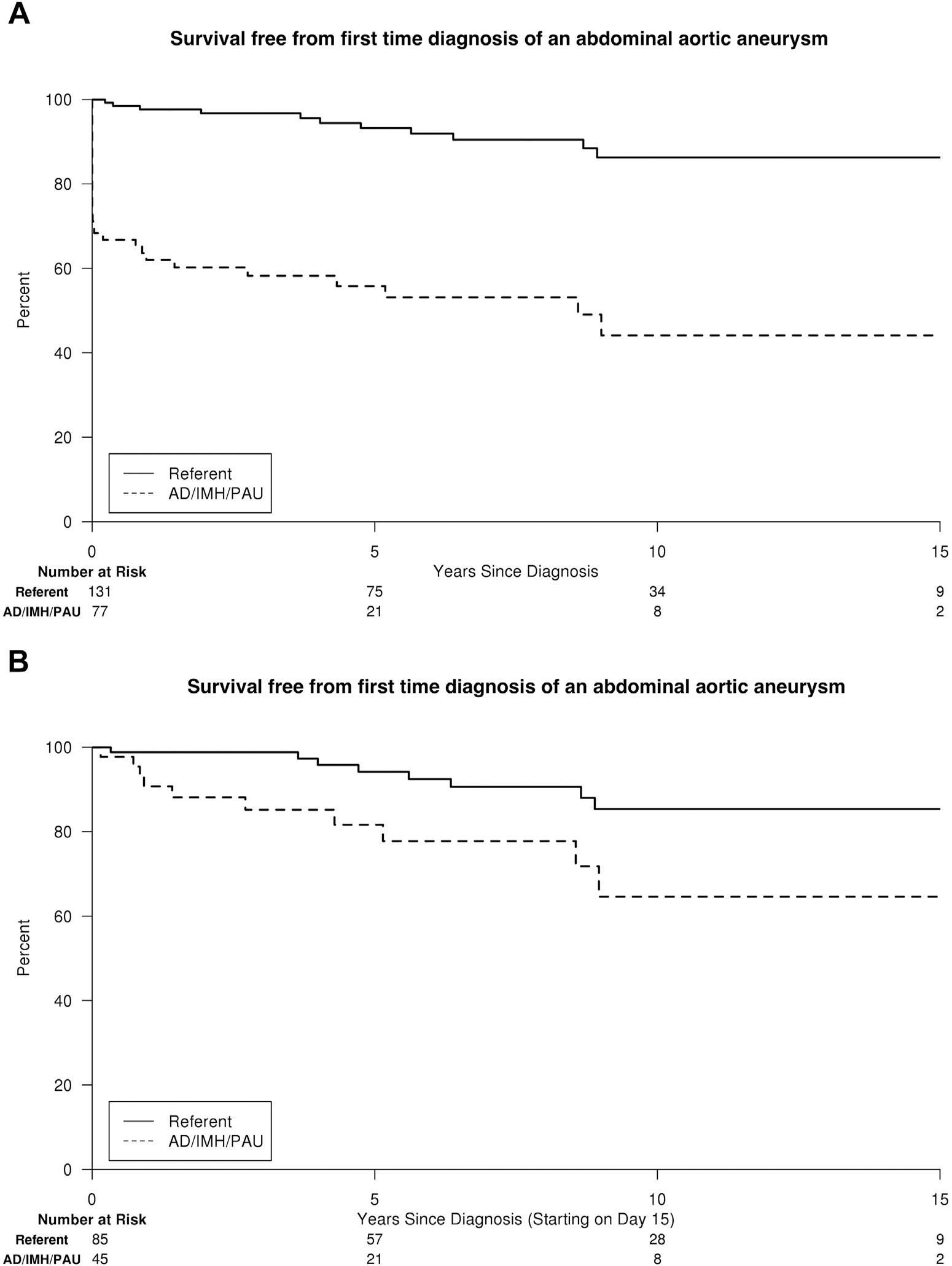
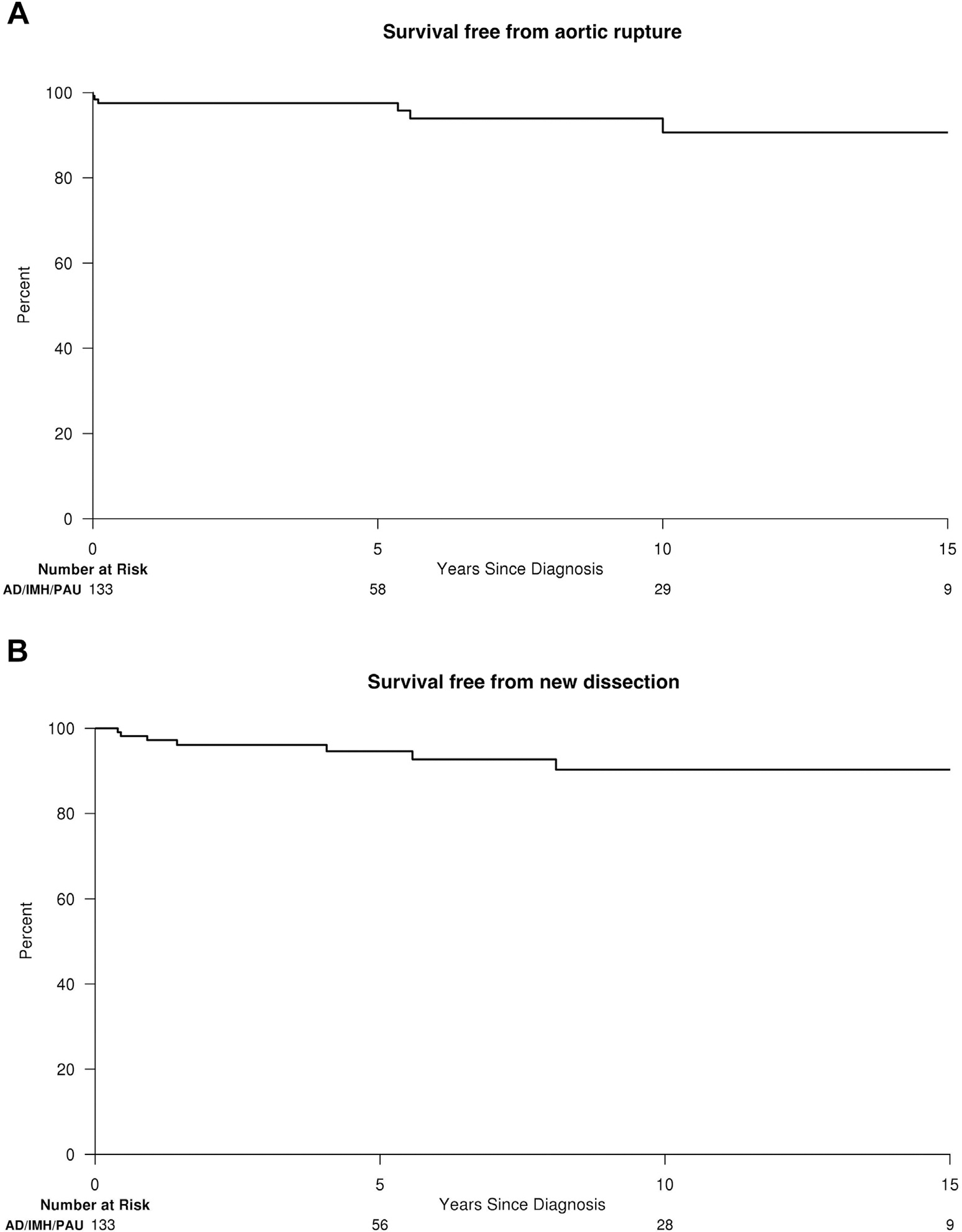
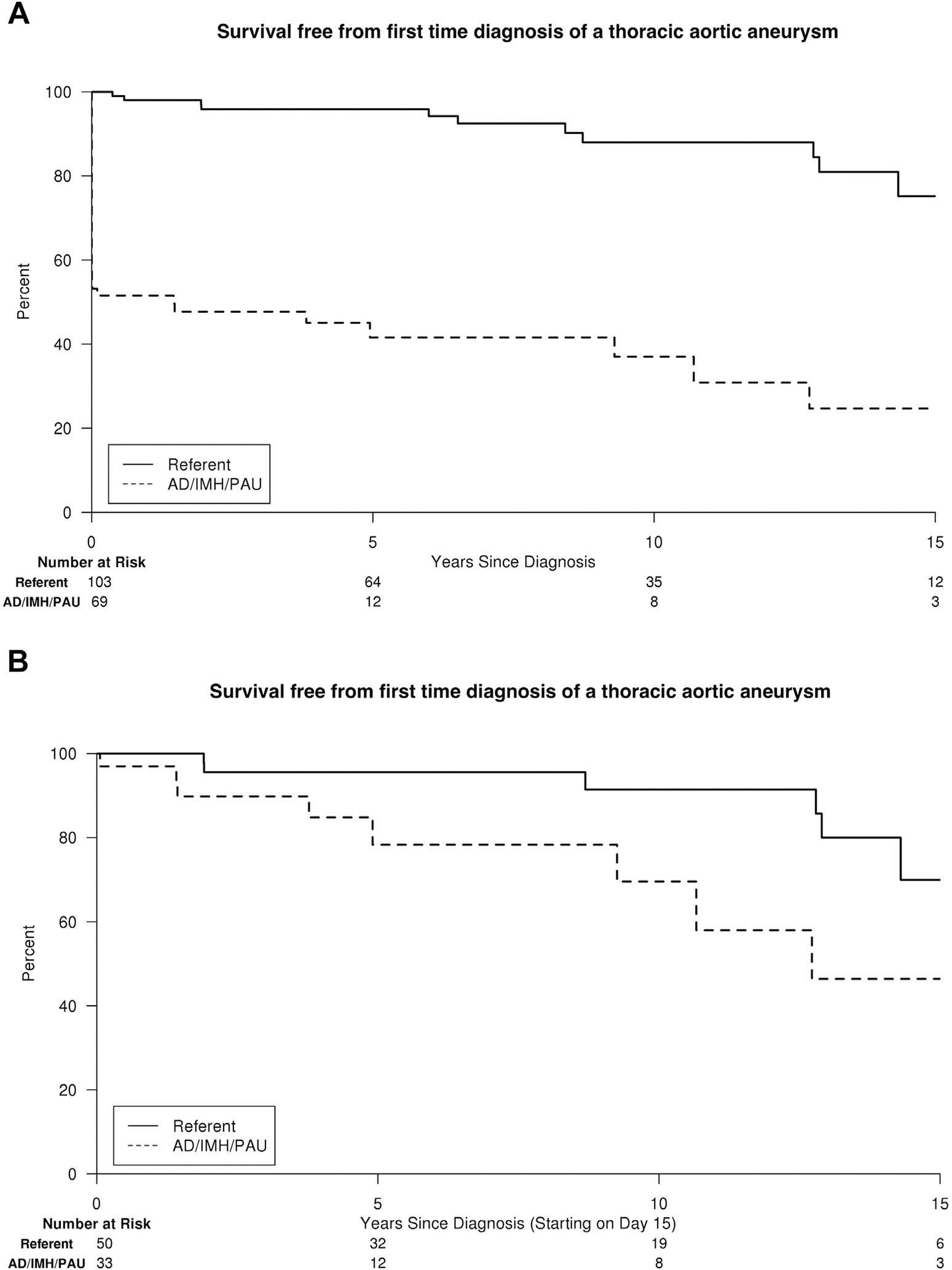
Retrospective review of an incident cohort of AD, IMH, and PAU patients in Olmsted County, Minnesota from 1995 to 2015. Primary end point was aortic death. Secondary end points were subsequent aortic events (aortic intervention, new dissection, or rupture not present at presentation) and first-time diagnosis of an aortic aneurysm. Outcomes were compared with randomly selected population referents matched for age and sex in a 3:1 ratio using Cox proportional hazards regression adjusting for comorbidities.
Among 133 patients (77 AD, 21 IMH, and 35 PAU), 57% were males, and mean age was 71.8 years (standard deviation, 14). Median follow-up was 10 years. Of 73 deaths among AD/IMH/PAU patients, 23 (32%) were aortic-related. Estimated freedom from aortic death was 84%, 80%, and 77% at 5, 10, and 15 years. There were no aortic deaths among population referents (adjusted hazard ratio [HR] for aortic death in AD/IMH/PAU, 184.7; 95% confidence interval [95% CI], 10.3-3,299.2; P < 0.001). Fifty (38%) AD/IMH/PAU patients had a subsequent aortic event (aortic intervention, new dissection, or rupture), whereas there were 8 (2%) aortic events among population referents (all elective aneurysm repairs; adjusted HR for any aortic event and aortic intervention in AD/IMH/PAU patients, 33.3; 95% CI, 15.3-72.0; P < 0.001 and 31.5; 95% CI, 14.5-68.4; P < 0.001, respectively). After excluding aortic events/interventions ≤14 days of diagnosis, AD/IMH/PAU patients remained at increased risk of any aortic event (adjusted HR, 10.8; 95% CI, 3.9-29.8; P < 0.001) and aortic intervention (adjusted HR, 9.6; 95% CI, 3.4-26.8; P < 0.001). Among those subjects with available follow-up imaging, the risk of first-time diagnosis of aortic aneurysm was significantly increased for AD/IMH/PAU patients when compared with population referents (adjusted HR, 10.9; 95% CI, 5.4-21.7; P < 0.001 and 8.3; 95% CI, 4.1-16.7; P < 0.001 for thoracic and abdominal aneurysms, respectively) and remained increased when excluding aneurysms that formed within 14 days of AD/IMH/PAU (adjusted HR, 6.2; 95% CI, 1.8-21.1; P = 0.004 and 2.8; 95% CI, 1.0-7.6; P = 0.040 for thoracic and abdominal aneurysms, respectively).
AD/IMH/PAU patients have a substantial risk of aortic death, any aortic event, aortic intervention, and first-time diagnosis of aortic aneurysm that persists even when the acute phase (≤14 days after diagnosis) is uncomplicated. Advances in postdiagnosis treatment are necessary to improve the prognosis in these patients.
本研究旨在从基于人群的角度分析主动脉夹层(AD)、壁内血肿(IMH)和穿透性主动脉溃疡(PAU)诊断后的主动脉相关结局。
对1995年至2015年明尼苏达州奥尔姆斯特德县AD、IMH和PAU患者的发病队列进行回顾性研究。主要终点是主动脉死亡。次要终点是随后的主动脉事件(主动脉干预、新的夹层或就诊时不存在的破裂)和首次诊断为主动脉瘤。使用Cox比例风险回归对合并症进行调整,将结局与按年龄和性别以3:1比例随机选择的人群对照进行比较。
在133例患者(77例AD、21例IMH和35例PAU)中,57%为男性,平均年龄为71.8岁(标准差14)。中位随访时间为10年。在AD/IMH/PAU患者的73例死亡中,23例(32%)与主动脉相关。5年、10年和15年时主动脉死亡的估计无事件生存率分别为84%、80%和77%。人群对照中无主动脉死亡(AD/IMH/PAU患者主动脉死亡的调整风险比[HR]为184.7;95%置信区间[95%CI]为10.3 - 3299.2;P < 0.001)。50例(38%)AD/IMH/PAU患者发生了随后的主动脉事件(主动脉干预、新的夹层或破裂),而人群对照中有8例(2%)发生主动脉事件(均为择期动脉瘤修复;AD/IMH/PAU患者任何主动脉事件和主动脉干预的调整HR分别为33.3;95%CI为15.3 - 72.0;P < 0.001和31.5;95%CI为14.5 - 68.4;P < 0.001)。排除诊断后≤14天的主动脉事件/干预后,AD/IMH/PAU患者发生任何主动脉事件(调整HR为10.8;95%CI为3.9 - 29.8;P < 0.001)和主动脉干预(调整HR为9.6;95%CI为3.4 - 26.8;P < 0.001)的风险仍然增加。在有可用随访影像学检查的受试者中,与人群对照相比,AD/IMH/PAU患者首次诊断为主动脉瘤的风险显著增加(调整HR为10.9;95%CI为5.4 - 21.7;P < 0.001,胸主动脉瘤和腹主动脉瘤分别为8.3;95%CI为4.1 - 16.7;P < 0.001),排除AD/IMH/PAU后14天内形成的动脉瘤后风险仍然增加(胸主动脉瘤和腹主动脉瘤的调整HR分别为6.2;95%CI为1.8 - 21.1;P = 0.004和2.8;95%CI为1.0 - 7.6;P = 0.040)。
AD/IMH/PAU患者有发生主动脉死亡、任何主动脉事件、主动脉干预和首次诊断为主动脉瘤的重大风险,即使急性期(诊断后≤14天)无并发症,该风险仍然存在。有必要改进诊断后的治疗方法以改善这些患者的预后。