Department of Infectious Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, No.1 Shuaifuyuan, Wangfujing Street, Beijing, 100730, China.
Department of International Medical Services, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, No.1 Shuaifuyuan, Wangfujing Street, Beijing, 100730, China.
Infect Dis Poverty. 2020 Jun 22;9(1):75. doi: 10.1186/s40249-020-00700-8.
It is not completely clear whether a very high pre-therapy viral load (≥ 500 000 copies/ml) can impair the virological response. The aim of this study was to examine the influence of very high baseline HIV-RNA levels on long-term virological responses under one type of regimen.
A retrospective study was performed based on data from two multicenter cohorts in China from January to November 2009, and from May 2013 to December 2015. Untreated HIV infected adults between 18 and 65 years old were recruited before receiving non-nucleoside reverse transcriptase inhibitor-based regimen. All patients had baseline HIV-RNA levels over 500 copies/ml, good adherence, and were followed for at least 24 weeks. Virological suppression was defined as the first HIV-RNA < 50 copies/ml. Virological failure was defined as any of incomplete viral suppression (HIV-RNA ≥ 200 copies/ml without virological suppression within 24 weeks of treatment) and viral rebound (confirmed HIV-RNA level ≥ 50 copies/ml after virological suppression). Chi-square test, Kaplan-Meier analysis, Cox proportional hazards model and Logistic regression were used to compare virological response between each pretreated viral load stratum.
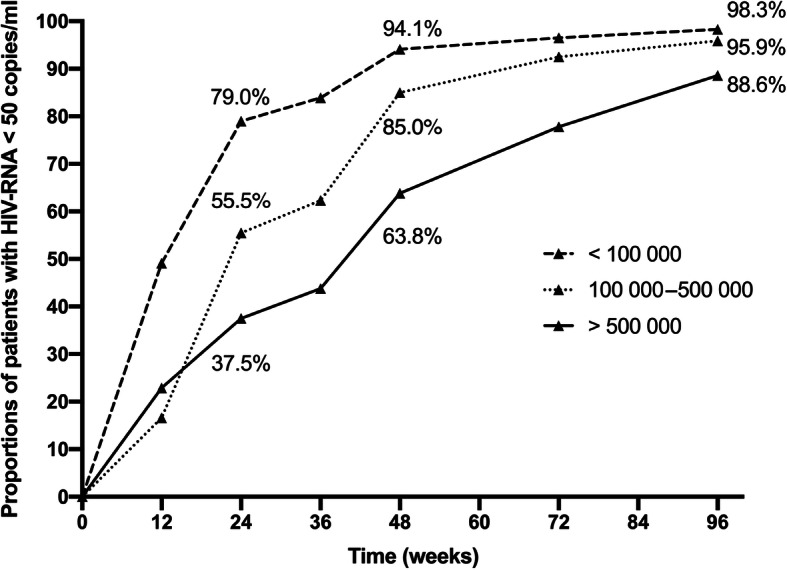
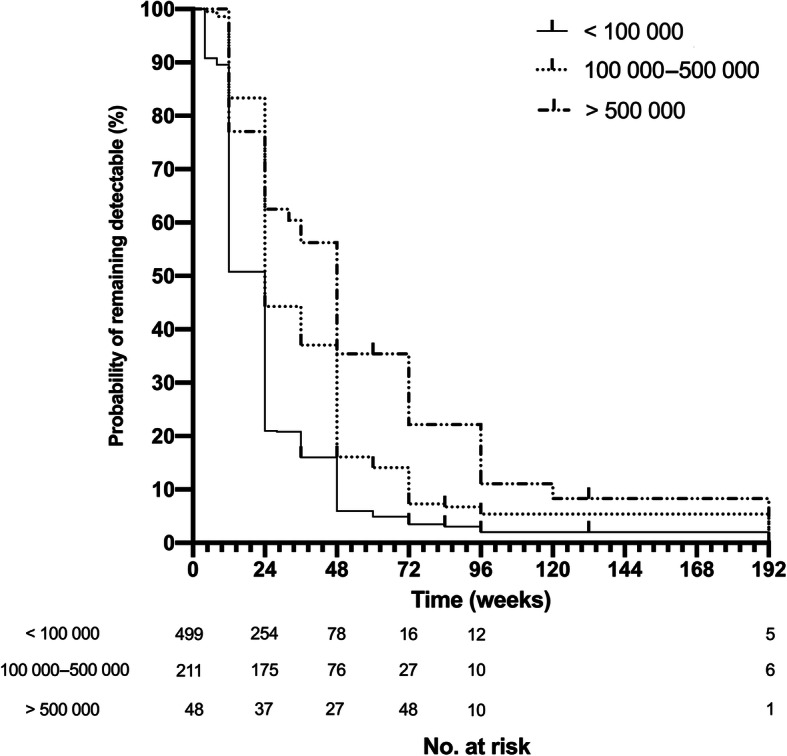
A total of 758 treatment-naïve HIV patients in China were enlisted. Median follow-up time (IQR) was 144 (108-276) weeks. By week 48, rates of virological suppression in three groups (< 100 000, 100 000-500 000 and ≥ 500 000 copies/ml) were 94.1, 85.0, and 63.8%, respectively (P < 0.001). Very high baseline HIV viremia over 500 000 copies/ml were found to be associated with delayed virological suppression (≥ 500 000 vs < 100 000, adjusted relative hazard = 0.455, 95% CI: 0.32-0.65; P < 0.001) as well as incomplete viral suppression (≥ 500 000 vs < 100 000, adjusted odds ratio [aOR] = 6.084, 95% CI: 2.761-13.407; P < 0.001) and viral rebound (≥ 50 000 vs < 100 000, aOR = 3.671, 95% CI: 1.009-13.355, P = 0.048).
Very high levels of pre-treatment HIV-RNA were related with delayed efficacy of NNRTI-based ART and increased risk of treatment failure. More potent initial regimens should be considered for those with this clinical character.
目前尚不清楚极高的基线病毒载量(≥500,000 拷贝/ml)是否会影响病毒学应答。本研究旨在考察在一种治疗方案下,基线 HIV RNA 水平极高对长期病毒学应答的影响。
本研究为回顾性研究,基于 2009 年 1 月至 11 月和 2013 年 5 月至 2015 年 12 月期间中国两个多中心队列的数据。招募未接受非核苷类逆转录酶抑制剂为基础的治疗方案的 18-65 岁 HIV 感染成人。所有患者的基线 HIV RNA 水平均超过 500 拷贝/ml,具有良好的依从性,随访至少 24 周。病毒学抑制定义为首次 HIV RNA<50 拷贝/ml。病毒学失败定义为任何一种不完全病毒抑制(治疗 24 周内 HIV RNA≥200 拷贝/ml 且未达到病毒学抑制)和病毒学反弹(病毒学抑制后确认 HIV RNA 水平≥50 拷贝/ml)。采用卡方检验、Kaplan-Meier 分析、Cox 比例风险模型和 Logistic 回归比较各预处理病毒载量分层的病毒学应答。
共纳入中国 758 例初治 HIV 患者。中位随访时间(IQR)为 144(108-276)周。第 48 周时,三组(<100,000、100,000-500,000 和≥500,000 拷贝/ml)的病毒学抑制率分别为 94.1%、85.0%和 63.8%(P<0.001)。极高的基线 HIV 病毒载量(>500,000 拷贝/ml)与病毒学抑制延迟(≥500,000 比<100,000,调整后的相对危险度=0.455,95%CI:0.32-0.65;P<0.001)以及不完全病毒抑制(≥500,000 比<100,000,调整后的比值比[aOR]=6.084,95%CI:2.761-13.407;P<0.001)和病毒学反弹(≥50,000 比<100,000,aOR=3.671,95%CI:1.009-13.355,P=0.048)相关。
极高的基线 HIV RNA 水平与 NNRTI 为基础的 ART 疗效延迟和治疗失败风险增加有关。对于具有这种临床特征的患者,应考虑使用更有效的初始治疗方案。