Department of Pediatrics, Ascension St. John Children's Hospital, Detroit, MI, USA.
Wayne State University, School of Medicine, Detroit, MI, USA.
Am J Case Rep. 2020 Jun 25;21:e923250. doi: 10.12659/AJCR.923250.
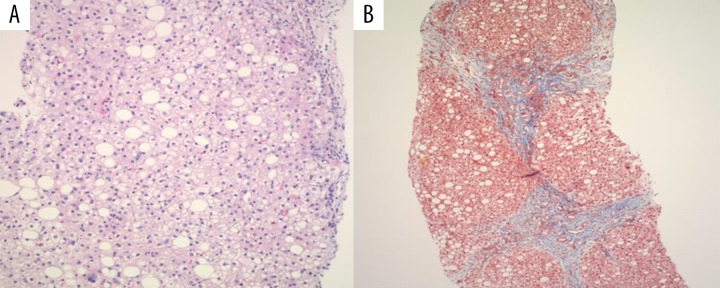
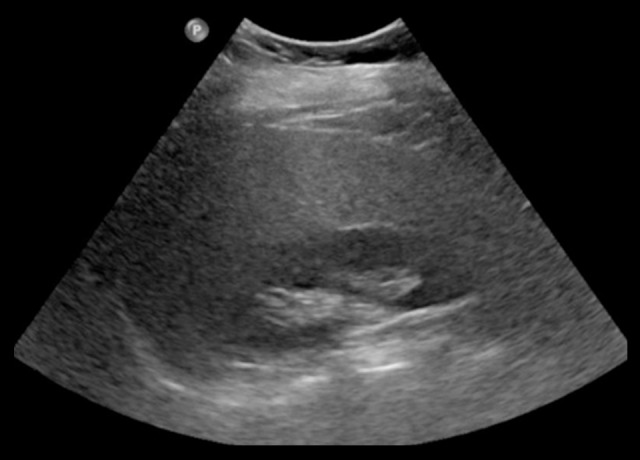
BACKGROUND Non-alcoholic fatty liver disease (NAFLD) is the presence of chronic hepatic steatosis in the absence of infections, steatogenic medication use, metabolic/genetic disorders, malnutrition, or ethanol consumption. NAFLD encompasses a spectrum of liver damage varying from non-alcoholic fatty liver (NAFL) on the most clinically benign end of the spectrum to cirrhosis on the opposite extreme, where most liver-related morbidity and mortality occurs. CASE REPORT We report a case of a 9-year-old boy with history of obesity (BMI 32.1 kg/m² - 99th percentile) and non-alcoholic fatty liver disease, who was referred to our pediatric gastroenterology clinic with a 1-week history of vomiting and right upper-quadrant abdominal pain. A review of the past medical history revealed transaminitis for the last 4 years and a dietary regimen for the last 2 years with poor compliance and follow-up. An extensive workup revealed an SGPT of 327 unit/L, SGOT 186 unit/L, and triglycerides of 208 mg/dL; infectious, metabolic, genetic, and autoimmune etiologies were ruled-out. The median liver stiffness measured by Fibroscan was 14 kPa, consistent with F4 fibrosis, and the cap median value was 271 dB/mW, reflective of S2 steatosis. An ultrasound-guided core liver biopsy revealed steatohepatitis with bridging and encircling fibrosis consistent with early/evolving cirrhosis. CONCLUSIONS Although cirrhosis is rarely seen in pediatric patients with NAFLD, it should always be considered. Secondly, Fibroscan, a non-invasive imaging procedure, is a useful tool to assess the level of fibrosis and steatosis in patients with NAFLD; early evaluation of our patient could potentially have limited the progression to cirrhosis.
非酒精性脂肪性肝病(NAFLD)是指在无感染、致肝脂肪变性药物使用、代谢/遗传紊乱、营养不良或乙醇摄入的情况下,肝脏出现慢性脂肪变性。NAFLD 涵盖了从最具临床良性的非酒精性脂肪肝(NAFL)到最极端的肝硬化的一系列肝损伤,大多数与肝脏相关的发病率和死亡率都发生在肝硬化。
我们报告了一例 9 岁肥胖男孩(BMI 32.1 kg/m² - 第 99 百分位)和非酒精性脂肪性肝病的病例,他因右季肋部疼痛和 1 周呕吐病史,被转至我院儿科胃肠病学门诊。回顾既往病史,发现过去 4 年有转氨基酶升高,过去 2 年有饮食方案,但依从性和随访不佳。广泛的检查显示 SGPT 为 327 U/L,SGOT 为 186 U/L,甘油三酯为 208 mg/dL;排除了感染、代谢、遗传和自身免疫病因。Fibroscan 测量的中位数肝硬度为 14 kPa,符合 F4 纤维化,CAP 中位数为 271 dB/mW,反映 S2 脂肪变性。超声引导下肝活检显示脂肪性肝炎伴桥接和环形纤维化,符合早期/进展性肝硬化。
虽然儿童 NAFLD 患者很少发生肝硬化,但应始终考虑到。其次,Fibroscan 是一种非侵入性成像检查,可用于评估 NAFLD 患者的纤维化和脂肪变性程度;对我们患者的早期评估可能会限制其进展为肝硬化。