University of Washington Medical Center, Seattle, Washington.
Duke Clinical Research Institute, Duke University, Durham, North Carolina.
J Am Coll Cardiol. 2020 Jun 30;75(25):3105-3118. doi: 10.1016/j.jacc.2020.04.065.
The CABANA (Catheter Ablation Versus Antiarrhythmic Drug Therapy for Atrial Fibrillation) trial randomized 2,204 patients with atrial fibrillation (AF) to catheter ablation or drug therapy. Analysis by intention-to-treat showed a nonsignificant 14% relative reduction in the primary outcome of death, disabling stroke, serious bleeding, or cardiac arrest.
The purpose of this study was to assess recurrence of AF in the CABANA trial.
The authors prospectively studied CABANA patients using a proprietary electrocardiogram recording monitor for symptom-activated and 24-h AF auto detection. The AF recurrence endpoint was any post-90-day blanking atrial tachyarrhythmias lasting 30 s or longer. Biannual 96-h Holter monitoring was used to assess AF burden. Patients who used the CABANA monitors and provided 90-day post-blanking recordings qualified for this analysis (n = 1,240; 56% of CABANA population). Treatment comparisons were performed using a modified intention-to-treat approach.
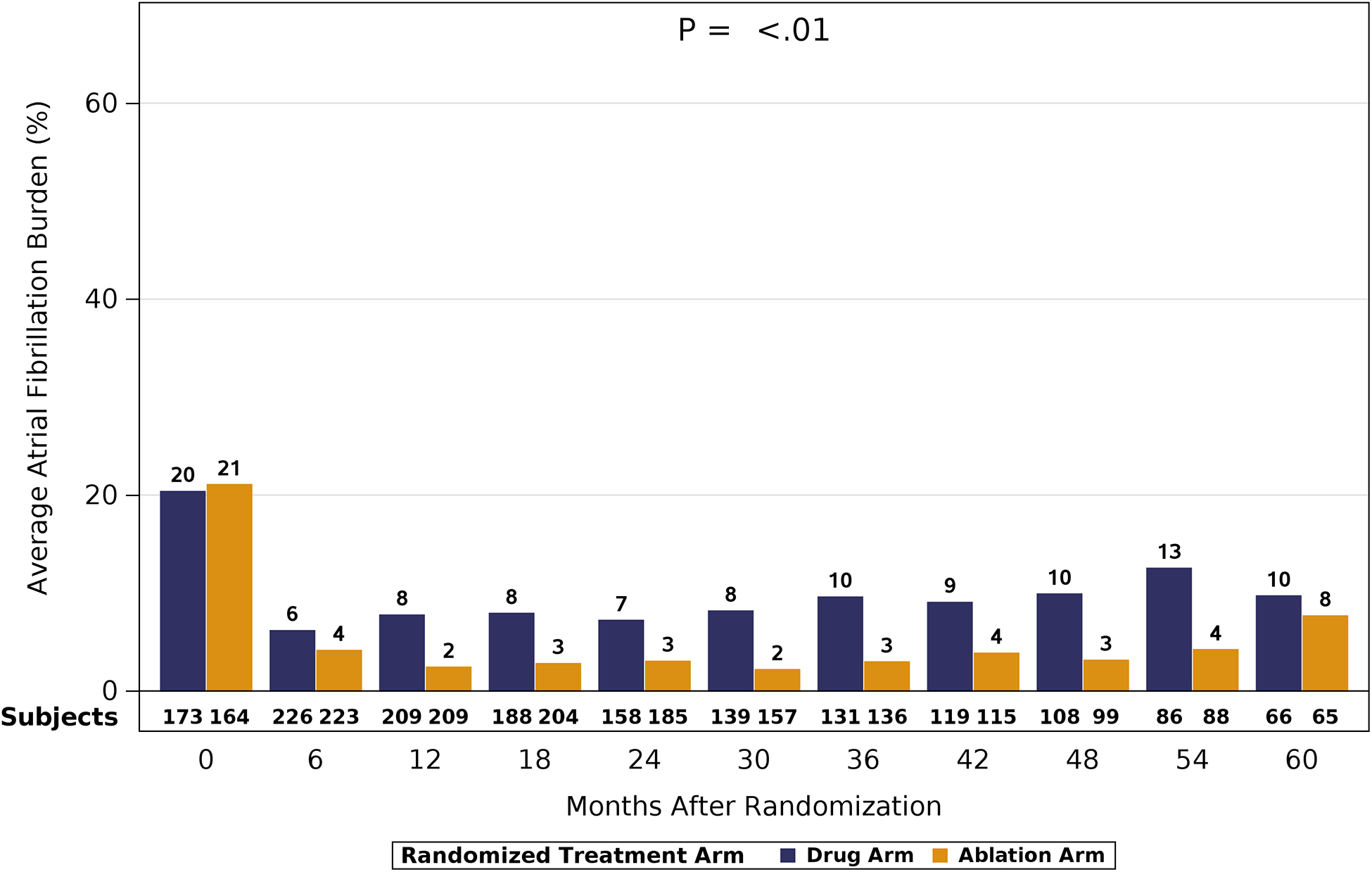
Median age of the 1,240 patients was 68 years, 34.4% were women, and AF was paroxysmal in 43.0%. Over 60 months of follow-up, first recurrence of any symptomatic or asymptomatic AF (hazard ratio: 0.52; 95% confidence interval: 0.45 to 0.60; p < 0.001) or first symptomatic-only AF (hazard ratio: 0.49; 95% confidence interval: 0.39 to 0.61; p < 0.001) were both significantly reduced in the catheter ablation group. Baseline Holter AF burden in both treatment groups was 48%. At 12 months, AF burden in ablation patients averaged 6.3%, and in drug-therapy patients, 14.4%. AF burden was significantly less in catheter ablation compared with drug-therapy patients across the 5-year follow-up (p < 0.001). These findings were not sensitive to the baseline pattern of AF.
Catheter ablation was effective in reducing recurrence of any AF by 48% and symptomatic AF by 51% compared with drug therapy over 5 years of follow-up. Furthermore, AF burden was also significantly reduced in catheter ablation patients, regardless of their baseline AF type. (Catheter Ablation vs Anti-arrhythmic Drug Therapy for Atrial Fibrillation Trial [CABANA]; NCT00911508).
CABANA(导管消融与抗心律失常药物治疗心房颤动)试验将 2204 例心房颤动(AF)患者随机分为导管消融或药物治疗组。意向治疗分析显示,主要终点(死亡、致残性卒中、严重出血或心脏骤停)的相对风险降低了 14%,但无统计学意义。
本研究旨在评估 CABANA 试验中 AF 的复发情况。
作者前瞻性地使用专有的心电图记录监测仪对 CABANA 患者进行监测,以检测症状激活和 24 小时 AF 自动检测。AF 复发终点为任何持续 30 秒或更长时间的 90 天后空白期房性心动过速。每 6 个月进行 96 小时动态心电图监测,以评估 AF 负荷。使用 CABANA 监测仪并提供 90 天空白期记录的患者符合本分析条件(n=1240;占 CABANA 人群的 56%)。采用改良意向治疗方法进行治疗比较。
1240 例患者的中位年龄为 68 岁,34.4%为女性,AF 为阵发性。在 60 多个月的随访中,导管消融组首次复发任何有症状或无症状 AF(风险比:0.52;95%置信区间:0.45 至 0.60;p<0.001)或首次有症状的单纯 AF(风险比:0.49;95%置信区间:0.39 至 0.61;p<0.001)的风险均显著降低。两组患者的基线 Holter AF 负荷均为 48%。在 12 个月时,消融患者的 AF 负荷平均为 6.3%,药物治疗患者的负荷为 14.4%。导管消融组在 5 年随访期间的 AF 负荷明显低于药物治疗组(p<0.001)。这些发现不受基线 AF 类型的影响。
与药物治疗相比,导管消融可有效降低 5 年内任何 AF 复发风险 48%,症状性 AF 复发风险 51%。此外,无论基线 AF 类型如何,导管消融患者的 AF 负荷也显著降低。(导管消融与抗心律失常药物治疗心房颤动试验[CABANA];NCT00911508)。