Unit of Biomarkers and Susceptibility, Oncology Data Analytics Program (ODAP), Catalan Institute of Oncology (ICO), Oncobell Program, Bellvitge Biomedical Research Institute (IDIBELL) and CIBERESP, L'Hospitalet de Llobregat, Barcelona, Spain.
Department of Clinical Sciences, Faculty of Medicine and Health Sciences, University of Barcelona, Barcelona, Spain.
J Immunother Cancer. 2020 Jun;8(1). doi: 10.1136/jitc-2019-000491.
Only certain disseminated cells are able to grow in secondary organs to create a metastatic tumor. Under the hypothesis that the immune microenvironment of the host tissue may play an important role in this process, we have categorized metastatic samples based on their immune features.
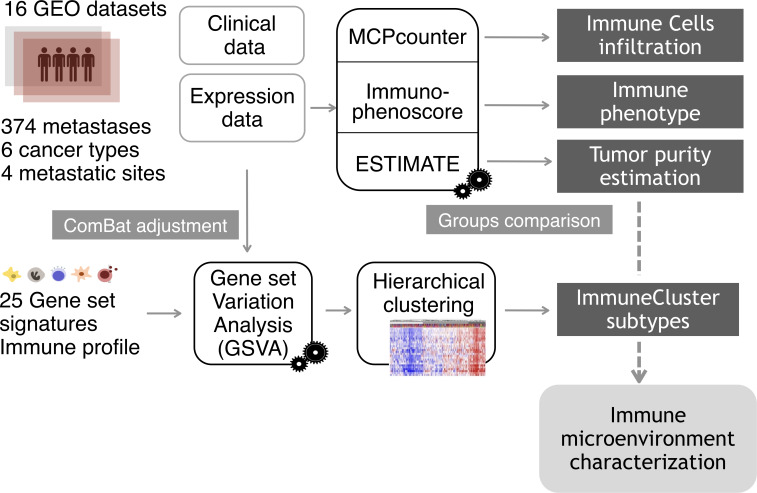
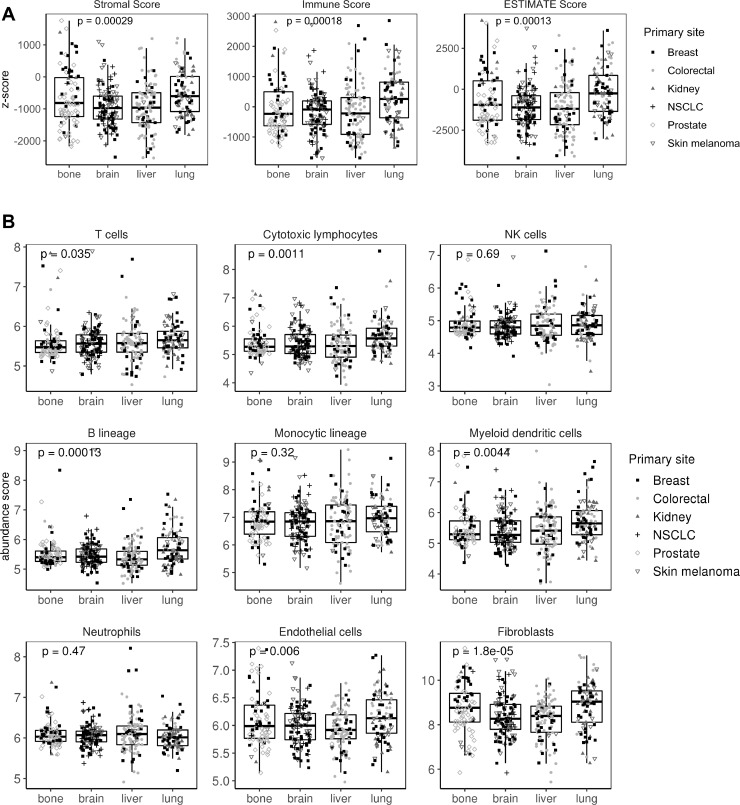
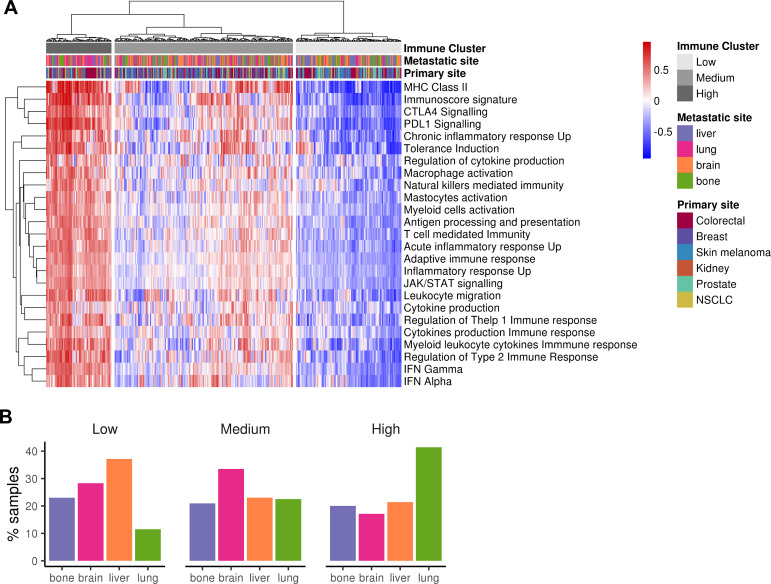
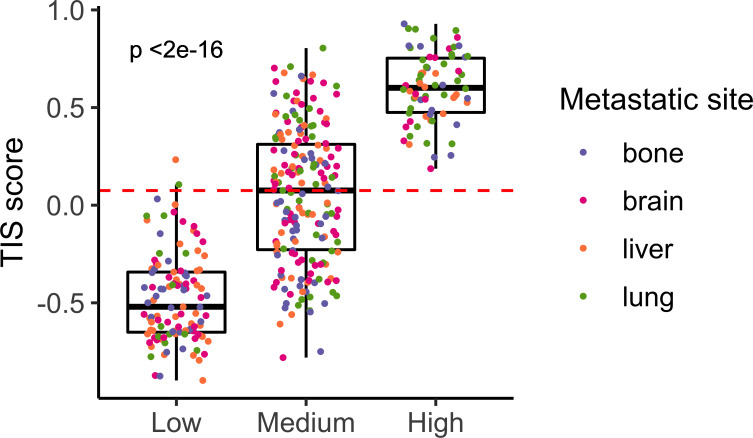
Gene expression data of metastatic samples (n=374) from four secondary sites (brain, bone, liver and lung) were used to characterize samples based on their immune and stromal infiltration using gene signatures and cell quantification tools. A clustering analysis was done that separated metastatic samples into three different immune categories: high, medium and low.
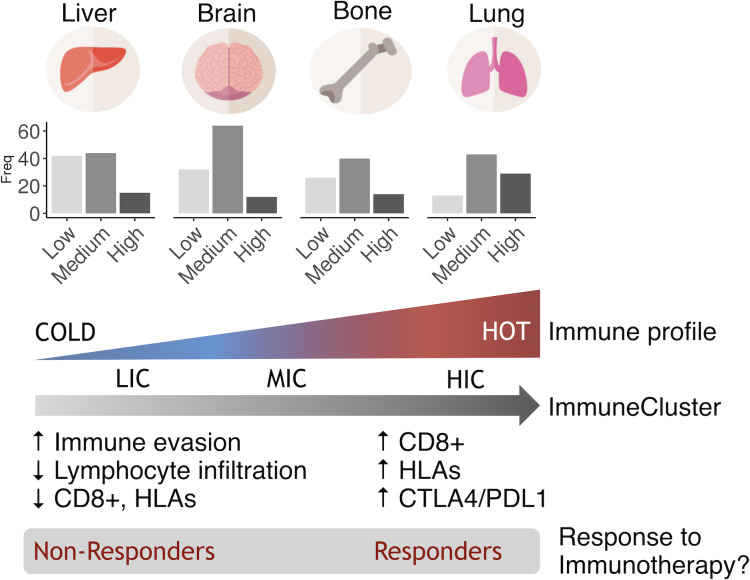
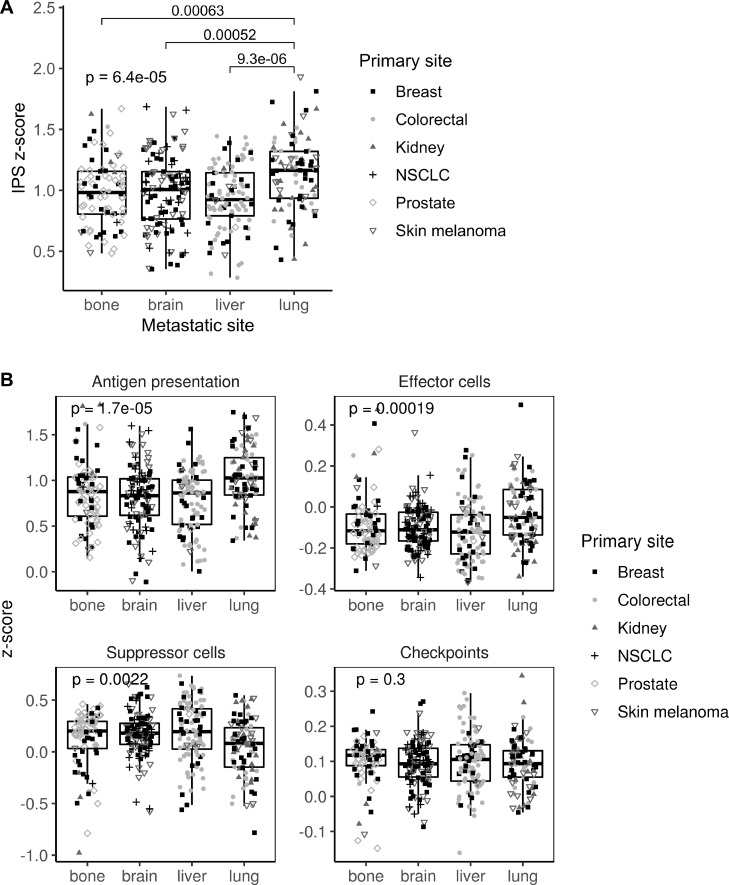
Significant differences were found between the immune profiles of samples metastasizing in distinct organs. Metastases in lung showed a higher immunogenic score than metastases in brain, liver or bone, regardless of their primary site of origin. Also, they preferentially clustered in the high immune group. Samples in this cluster exhibited a clear inflammatory phenotype, higher levels of immune infiltrate, overexpression of programmed death-ligand 1 (PD-L1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA4) pathways and upregulation of genes predicting clinical response to programmed cell death protein 1 (PD-1) blockade (T-cell inflammatory signature). A decision tree algorithm was used to select CD74 as a biomarker that identify samples belonging to this high-immune subtype of metastases, having specificity of 0.96 and sensitivity of 1.
We have found a group of lung-enriched metastases showing an inflammatory phenotype susceptible to be treated with immunotherapy.
只有某些播散细胞能够在次级器官中生长,从而形成转移性肿瘤。基于宿主组织的免疫微环境可能在这一过程中发挥重要作用的假设,我们根据免疫特征对转移性样本进行了分类。
使用来自四个次级部位(脑、骨、肝和肺)的转移性样本(n=374)的基因表达数据,使用基因特征和细胞定量工具,根据免疫和基质浸润对样本进行特征描述。进行聚类分析,将转移性样本分为三种不同的免疫类别:高、中、低。
不同器官转移的样本之间的免疫特征存在显著差异。无论其原发部位如何,肺转移的免疫评分均高于脑、肝或骨转移。此外,它们优先聚类在高免疫组。该聚类中的样本表现出明显的炎症表型,免疫浸润水平更高,程序性死亡配体 1(PD-L1)和细胞毒性 T 淋巴细胞相关蛋白 4(CTLA4)途径的过表达,以及预测对程序性细胞死亡蛋白 1(PD-1)阻断治疗有临床反应的基因上调(T 细胞炎症特征)。决策树算法用于选择 CD74 作为鉴定属于这种高免疫型转移性样本的生物标志物,其特异性为 0.96,敏感性为 1。
我们发现了一组富含肺的转移性肿瘤,它们表现出炎症表型,可能对免疫治疗敏感。