Department of Infection, Immunity and Inflammation, University of Leicester, University Road, Leicester LE1 7RH, UK.
Department of Infection, Immunity and Inflammation, Transplant Group, University of Leicester, Leicester General Hospital, Leicester LE5 4PW, UK.
Medicina (Kaunas). 2020 Jun 26;56(6):317. doi: 10.3390/medicina56060317.
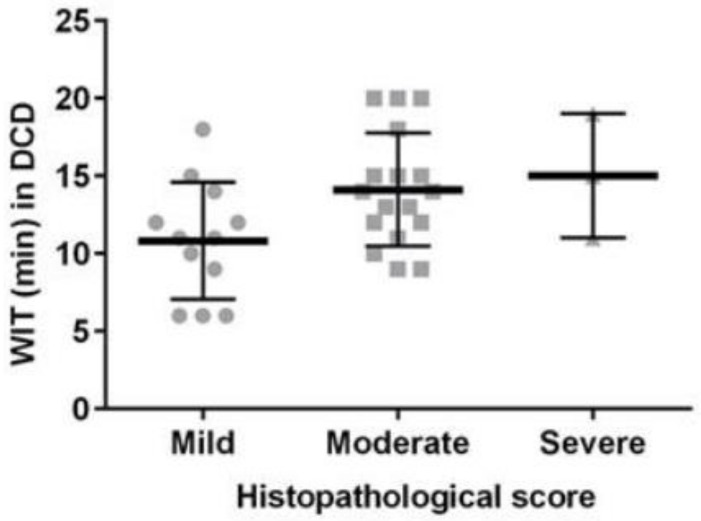
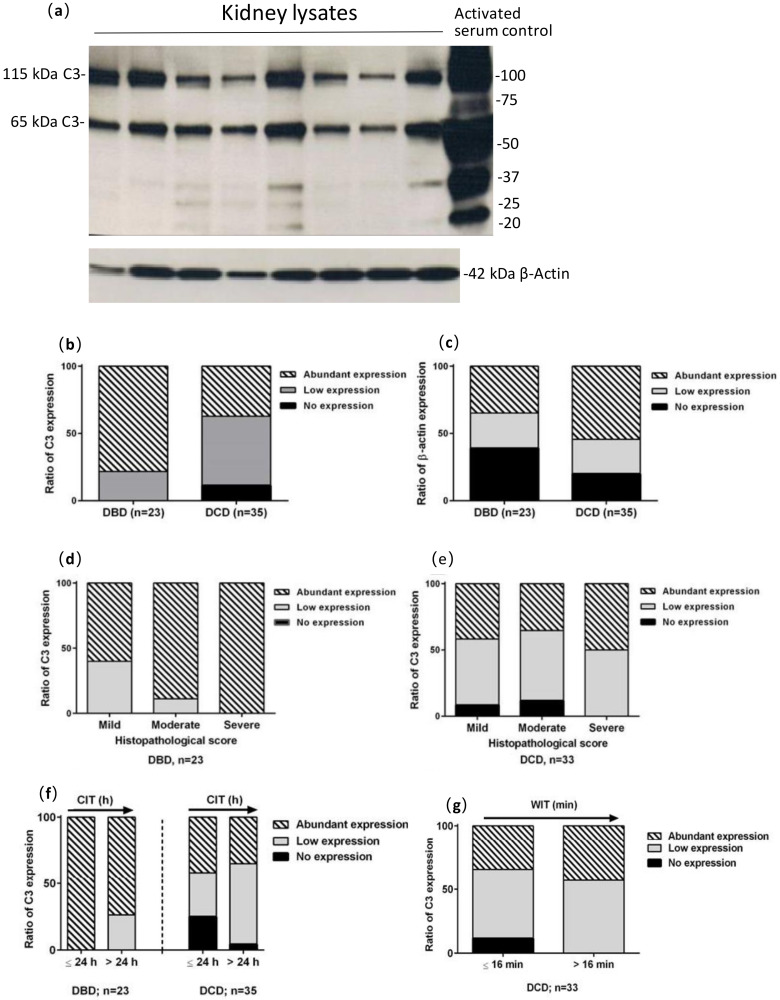
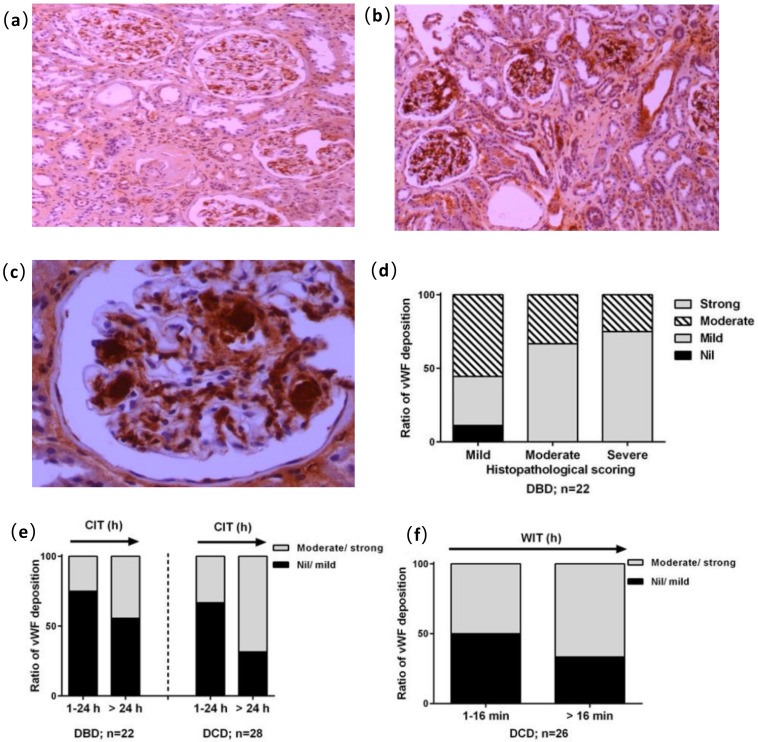
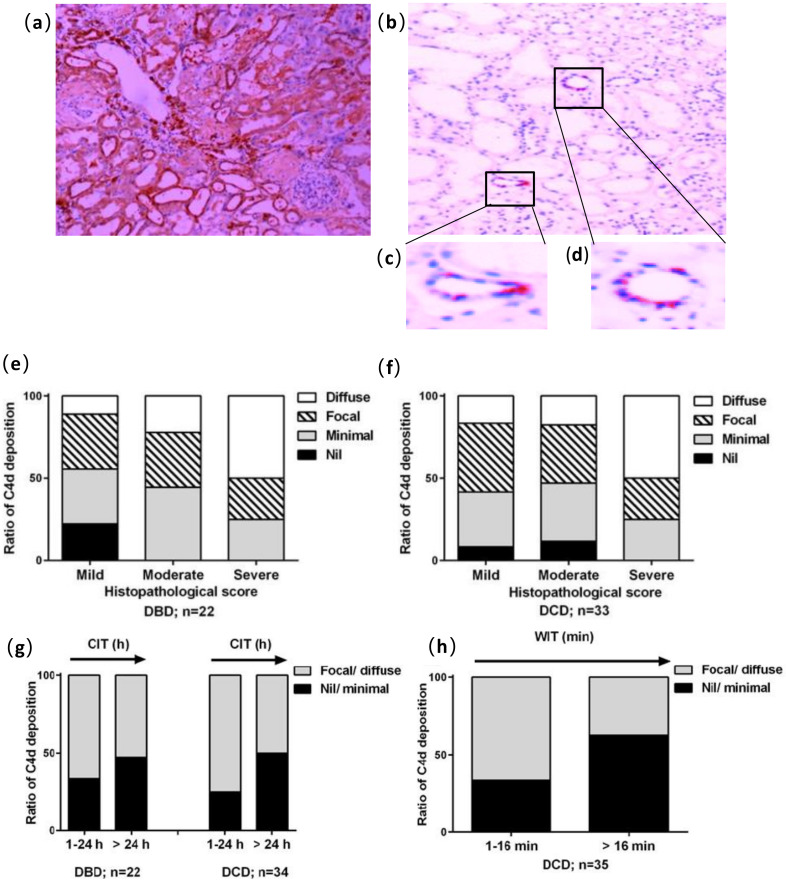
Kidneys from donation after circulatory death (DCD) are more likely to be declined for transplantation compared with kidneys from donation after brain death (DBD). The aim of this study was to evaluate characteristics in the biopsies of human DCD and DBD kidneys that were declined for transplantation in order to rescue more DCD kidneys. Sixty kidney donors (DCD = 36, DBD = 24) were recruited into the study and assessed using donor demographics. Kidney biopsies taken post cold storage were also evaluated for histological damage, inflammation (myeloperoxidase, MPO), von Willebrand factor (vWF) expression, complement 4d (C4d) deposition and complement 3 (C3) activation using H&E and immunohistochemistry staining, and Western blotting. More DBD donors (16/24) had a history of hypertension compared with DCDs (8/36, = 0.001). The mean warm ischemic time in the DCD kidneys was 12.9 ± 3.9 min. The mean cold ischemic time was not significantly different between the two groups of kidney donors (DBD 33.3 ± 16.7 vs. DCD 28.6 ± 14.1 h, > 0.05). The score of histological damage and MPO, as well as the reactivity of vWF, C4d and C3, varied between kidneys, but there was no significant difference between the two donor types ( > 0.05). However, vWF reactivity might be an early indicator for loss of tissue integrity, while C4d deposition and activated C3 might be better predictors for histological damage. Similar characteristics of DCD were shown in comparison with DBD kidneys. Importantly, the additional warm ischemic time in DCD appeared to have no further detectable adverse effects on tissue injury, inflammation and complement activation. vWF, C4d and C3 might be potential biomarkers facilitating the evaluation of donor kidneys.
与脑死亡供体(DBD)来源的肾脏相比,来自循环死亡供体(DCD)的肾脏更有可能被拒绝用于移植。本研究旨在评估因移植而被拒绝的人类 DCD 和 DBD 肾脏活检的特征,以便挽救更多的 DCD 肾脏。
60 名肾脏供体(DCD = 36,DBD = 24)被纳入研究,并根据供体人口统计学进行评估。还评估了冷储存后采集的肾脏活检标本的组织损伤、炎症(髓过氧化物酶,MPO)、血管性血友病因子(vWF)表达、补体 4d(C4d)沉积和补体 3(C3)激活情况,使用 H&E 和免疫组织化学染色和 Western blot。与 DCD 相比,更多的 DBD 供体(16/24)有高血压病史(DCD 为 8/36, = 0.001)。DCD 肾脏的平均热缺血时间为 12.9 ± 3.9 分钟。两组供体肾脏的冷缺血时间无显著差异(DBD 33.3 ± 16.7 vs. DCD 28.6 ± 14.1 h, > 0.05)。组织损伤评分和 MPO 以及 vWF、C4d 和 C3 的反应性在肾脏之间存在差异,但两种供体类型之间无显著差异( > 0.05)。然而,vWF 反应性可能是组织完整性丧失的早期指标,而 C4d 沉积和激活的 C3 可能是组织损伤的更好预测指标。与 DBD 肾脏相比,DCD 具有相似的特征。重要的是,DCD 中额外的热缺血时间似乎对组织损伤、炎症和补体激活没有进一步的可检测到的不利影响。vWF、C4d 和 C3 可能是有助于评估供体肾脏的潜在生物标志物。