Yue Hongli, Zhou Man, Lu Yu, Chen Liang, Cui Weihua
Department of Anesthesiology, Beijing Tian Tan Hospital, Capital Medical University, Beijing, People's Republic of China.
J Pain Res. 2020 Jun 12;13:1401-1410. doi: 10.2147/JPR.S249359. eCollection 2020.
Patients undergoing intraspinal tumor resection usually experience severe acute pain, delaying postoperative rehabilitation, and increasing incidence of chronic pain. Recently, an increasing number of studies have found that low-dose intravenous lidocaine infusion during and/or after surgery can reduce opioid usage and the incidence of related side effects, inhibit hyperalgesia and promote recovery. Thus far, no studies have evaluated the analgesic effect and safety of perioperative intravenous lidocaine infusion for intraspinal tumor resection, especially the long-term analgesic effects of patient-controlled analgesia (PCA) with lidocaine during the first postoperative 48 hours. This study tests the hypothesis that intra- and postoperative systemic lidocaine infusion for patients undergoing intraspinal tumor resection can relieve postoperative acute or chronic pain and reduce the opioid dosage and incidence of related side effects without other problems.
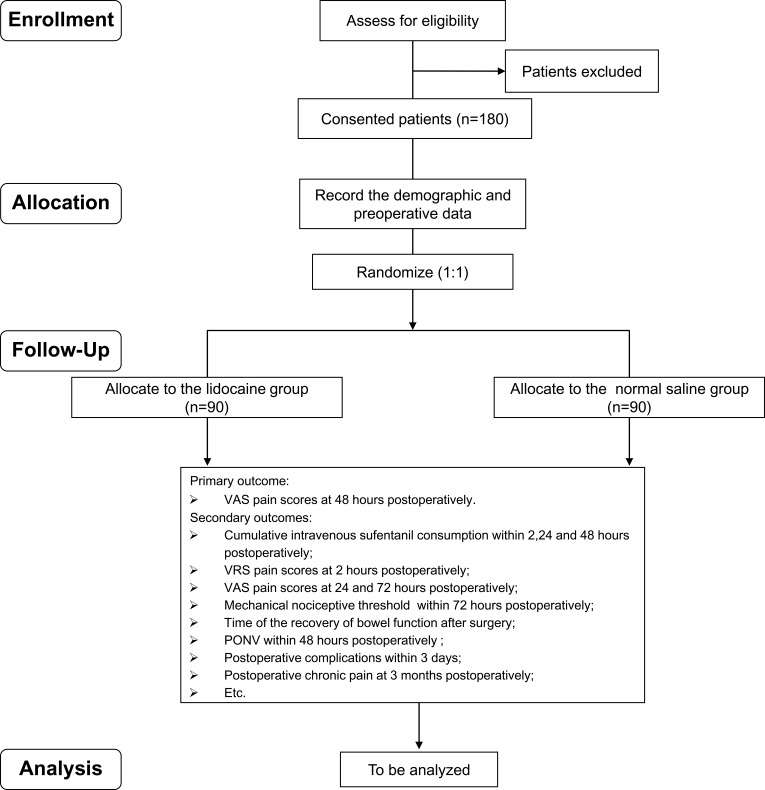
This is a prospective, randomized, placebo-controlled, and double-blinded study. In total, 180 participants scheduled for intraspinal tumor resection will be randomly divided into lidocaine and placebo groups. The lidocaine group will be administered lidocaine intravenously during anesthesia and postoperative pain management during the first 48 postoperative hours; the placebo group will be administered normal saline at the same volume, infusion rate, and timing. The primary outcome will be the postoperative visual analog scale (VAS) score. Secondary outcomes will be postoperative cumulative sufentanil consumption, indicators of postoperative recovery, and the incidence of perioperative adverse events.
This study investigates the effect of continuous intravenous lidocaine infusion on postoperative sufentanil consumption and VAS scores. The findings will provide a new strategy of anesthesia and analgesia management for intraspinal tumor resection.
接受脊髓肿瘤切除术的患者通常会经历严重的急性疼痛,这会延迟术后康复并增加慢性疼痛的发生率。最近,越来越多的研究发现,手术期间和/或术后低剂量静脉输注利多卡因可减少阿片类药物的使用及相关副作用的发生率,抑制痛觉过敏并促进恢复。迄今为止,尚无研究评估围手术期静脉输注利多卡因对脊髓肿瘤切除术的镇痛效果和安全性,尤其是术后48小时内利多卡因患者自控镇痛(PCA)的长期镇痛效果。本研究检验以下假设:接受脊髓肿瘤切除术的患者在术中和术后全身输注利多卡因可缓解术后急性或慢性疼痛,减少阿片类药物用量及相关副作用的发生率,且无其他问题。
这是一项前瞻性、随机、安慰剂对照、双盲研究。总共180名计划接受脊髓肿瘤切除术的参与者将被随机分为利多卡因组和安慰剂组。利多卡因组将在麻醉期间及术后48小时的疼痛管理期间静脉输注利多卡因;安慰剂组将输注相同体积、输注速率和时间的生理盐水。主要结局指标将是术后视觉模拟评分(VAS)。次要结局指标将是术后舒芬太尼累积用量、术后恢复指标以及围手术期不良事件的发生率。
本研究调查持续静脉输注利多卡因对术后舒芬太尼用量和VAS评分的影响。研究结果将为脊髓肿瘤切除术的麻醉和镇痛管理提供一种新策略。