From the Division of Epilepsy and Clinical Neurophysiology (I.S.F., M.A.-G., C.B.A., J.C., M.G.-L., A.V., T.L.), Department of Neurology, and Department of Neurology (R.C.T.), Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children's Hospital, Harvard Medical School, MA; Department of Child Neurology (I.S.F.), Hospital Sant Joan de Déu, Universitat de Barcelona, Spain; Division of Neurology (N.S.A.), Departments of Neurology and Pediatrics, Children's Hospital of Philadelphia and University of Pennsylvania; Pediatric Neurology Unit (M.A.-G.), Department of Pediatrics, Hospital Universitari Son Espases, Universitat de les Illes Balears, Palma, Spain; Section of Pediatric Critical Care Medicine (A.A., Y.-C.L.), Department of Pediatrics, Baylor College of Medicine, Houston, TX; Division of Neurology (R.A., T.G., K.P.), Cincinnati Children's Hospital Medical Center, University of Cincinnati, OH; University of Virginia Health (J.N.B., H.P.G.), Charlottesville; Center for Neuroscience (J.L.C., W.D.G.), Children's National Medical Center, George Washington University School of Medicine and Health Sciences, Washington, DC; Departments of Pediatrics and Neurology (K.E.C.), Children's Hospital Colorado, University of Colorado School of Medicine, Aurora; Department of Pediatric Neurology (R.F.-M., K.S.), Children's Hospital of Wisconsin, Medical College of Wisconsin, Milwaukee; Instituto de Pediatría (M.G.-L.), Facultad de Medicina, Universidad Austral de Chile, Valdivia, Chile; Servicio de Neuropsiquiatría Infantil (M.G.-L.), Hospital Clínico San Borja Arriarán, Universidad de Chile, Santiago; Ruth D. & Ken M. Davee Pediatric Neurocritical Care Program (J.G., T.M.), Northwestern University Feinberg School of Medicine, Chicago, IL; Division of Pediatric and Developmental Neurology (R.M.G.), Department of Neurology, Washington University School of Medicine, St. Louis, MO; Division of Pediatric Neurology (M.A.M., D.T.), Duke University Medical Center, Duke University, Durham, NC; Department of Pediatrics and Neurology (L.A.M., E.N., M.S.W.), Seattle Children's Hospital, University of Washington; Center for Integrative Brain Research (L.A.M., E.N., M.S.W.), Seattle Children's Research Institute, WA; Department of Neurology (E.P.), Mayo Clinic, Mayo Clinic School of Medicine, Rochester, MN; Department of Neurology (J.P.), Doernbercher Children's Hospital, Oregon Health & Science University, Portland; Department of Neurology (A.O.), Nationwide Children's Hospital, Ohio State University, Columbus; Division of Child Neurology and Institute for Genomic Medicine (T.T.S.), Columbia University Irving Medical Center, New York Presbyterian Hospital, New York; Division of Critical Care Medicine (A.A.T.), The Children's Hospital of Philadelphia, Perelman School of Medicine at the University of Pennsylvania; Division of Child and Adolescent Neurology (A.V.), Department of Neurology, Mayo Clinic, Rochester, MN; Barrow Neurological Institute (A.W., K.W.), Phoenix Children's Hospital; and Department of Pediatrics (A.W., K.W.), University of Arizona School of Medicine, Phoenix.
Neurology. 2020 Sep 1;95(9):e1222-e1235. doi: 10.1212/WNL.0000000000010174. Epub 2020 Jul 1.
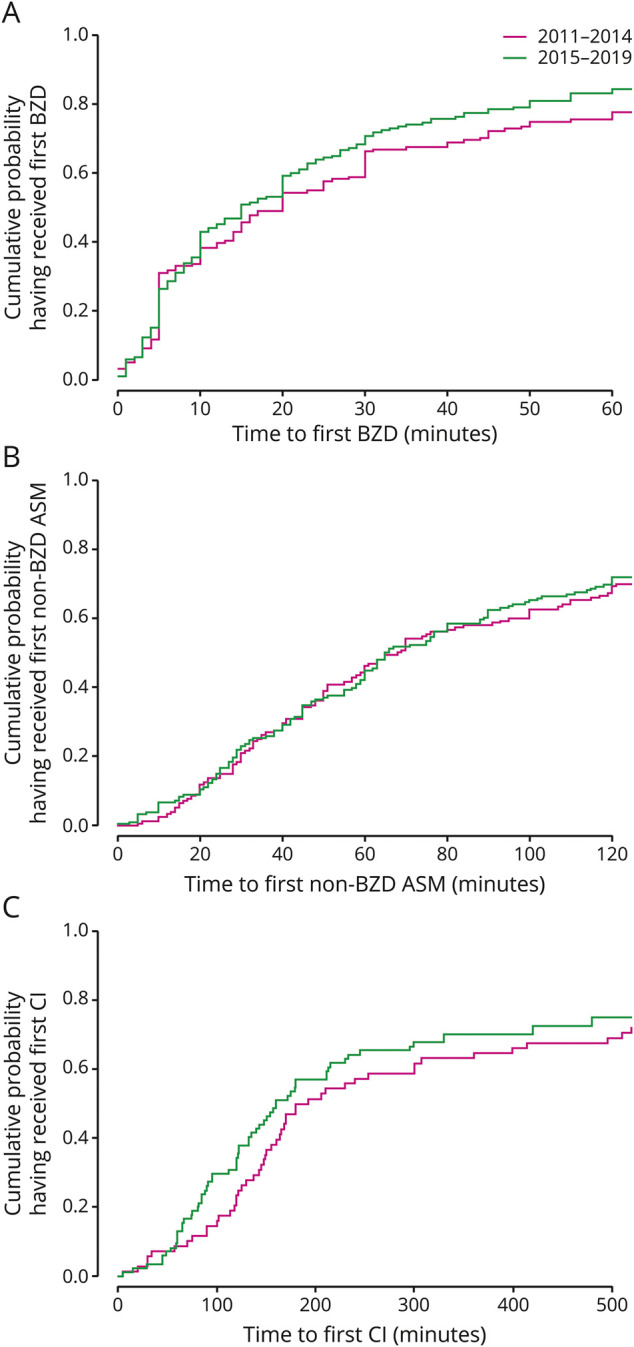
To determine whether publication of evidence on delays in time to treatment shortens time to treatment in pediatric refractory convulsive status epilepticus (rSE), we compared time to treatment before (2011-2014) and after (2015-2019) publication of evidence of delays in treatment of rSE in the Pediatric Status Epilepticus Research Group (pSERG) as assessed by patient interviews and record review.
We performed a retrospective analysis of a prospectively collected dataset from June 2011 to September 2019 on pediatric patients (1 month-21 years of age) with rSE.
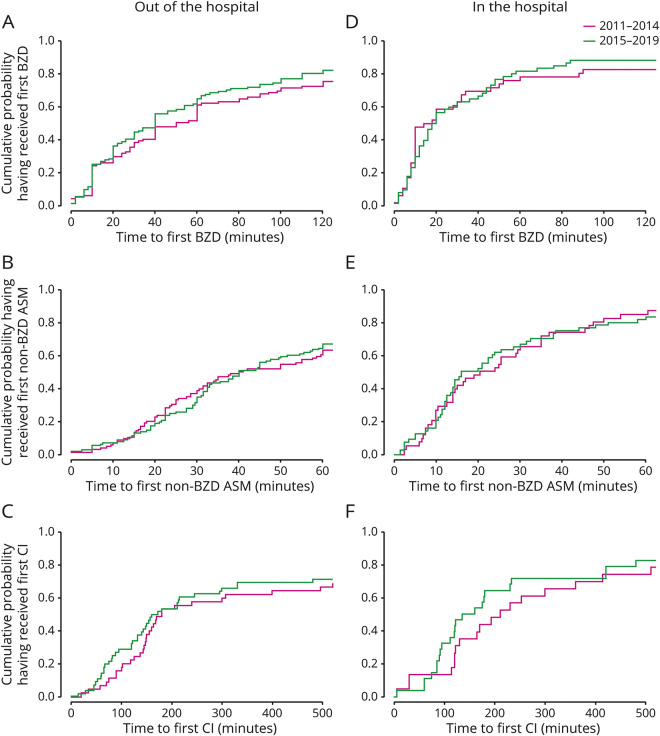
We studied 328 patients (56% male) with median (25th-75th percentile [p-p]) age of 3.8 (1.3-9.4) years. There were no differences in the median (p-p) time to first benzodiazepine (BZD) (20 [5-52.5] vs 15 [5-38] minutes, = 0.3919), time to first non-BZD antiseizure medication (68 [34.5-163.5] vs 65 [33-142] minutes, = 0.7328), and time to first continuous infusion (186 [124.2-571] vs 160 [89.5-495] minutes, = 0.2236). Among 157 patients with out-of-hospital onset whose time to hospital arrival was available, the proportion who received at least 1 BZD before hospital arrival increased after publication of evidence of delays (41 of 81 [50.6%] vs 57 of 76 [75%], = 0.0018), and the odds ratio (OR) was also increased in multivariable logistic regression (OR 4.35 [95% confidence interval 1.96-10.3], = 0.0005).
Publication of evidence on delays in time to treatment was not associated with improvements in time to treatment of rSE, although it was associated with an increase in the proportion of patients who received at least 1 BZD before hospital arrival.
为了确定延迟治疗的证据发布是否会缩短儿科难治性惊厥性癫痫持续状态(rSE)的治疗时间,我们比较了在儿科学癫痫持续状态研究组(pSERG)中,在发布 rSE 治疗延迟的证据前后(2015-2019 年),通过患者访谈和记录回顾评估的治疗时间。
我们对 2011 年 6 月至 2019 年 9 月期间前瞻性收集的儿科患者(1 个月至 21 岁)的数据集进行了回顾性分析。
我们研究了 328 名患者(56%为男性),中位数(25 至 75 百分位数 [p-p])年龄为 3.8 岁(1.3-9.4 岁)。首次苯二氮䓬(BZD)的中位数(p-p)时间没有差异(20 [5-52.5] 与 15 [5-38] 分钟, = 0.3919),首次非 BZD 抗惊厥药物的中位数(p-p)时间也没有差异(68 [34.5-163.5] 与 65 [33-142] 分钟, = 0.7328),首次连续输注的中位数(p-p)时间也没有差异(186 [124.2-571] 与 160 [89.5-495] 分钟, = 0.2236)。在 157 名有院外发病且可获得入院时间的患者中,在发布延迟治疗证据后,至少接受 1 次 BZD 治疗的患者比例增加(81 例中的 41 例[50.6%]与 76 例中的 57 例[75%], = 0.0018),并且多变量逻辑回归中的比值比(OR)也增加(OR 4.35 [95%置信区间 1.96-10.3], = 0.0005)。
尽管发布关于治疗时间延迟的证据与至少有 1 次 BZD 在入院前接受治疗的患者比例增加有关,但它与儿科难治性惊厥性癫痫持续状态的治疗时间改善无关。