Division of Thoracic Surgery, Taichung Veterans General Hospital, 1650, Taiwan Boulevard Sect. 4, Taichung, Taiwan.
Institute of Clinical Medicine, National Yang-Ming University, Taipei, Taiwan.
J Med Case Rep. 2020 Jul 7;14(1):106. doi: 10.1186/s13256-020-02391-z.
Neoadjuvant chemoradiotherapy is currently the gold standard treatment for esophageal cancer prior to surgery. This radiation therapy will sometimes lead to liver damage parallel to esophageal lesions, which mimics liver metastasis visualized by F-fluorodeoxyglucose positron emission tomography with computed tomography. In this report, we publish virtual radiation-induced liver damage images obtained during surgery, along with the coherent pathology, in order to confirm the false-positive result through an optimally decisive radiological examination.
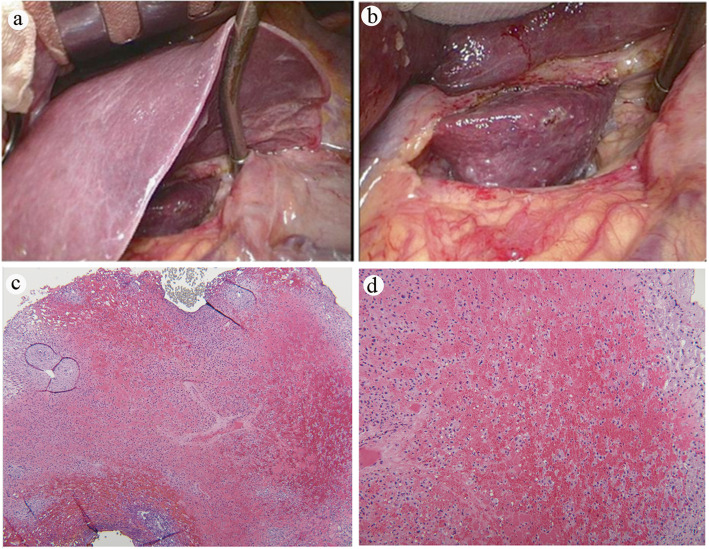
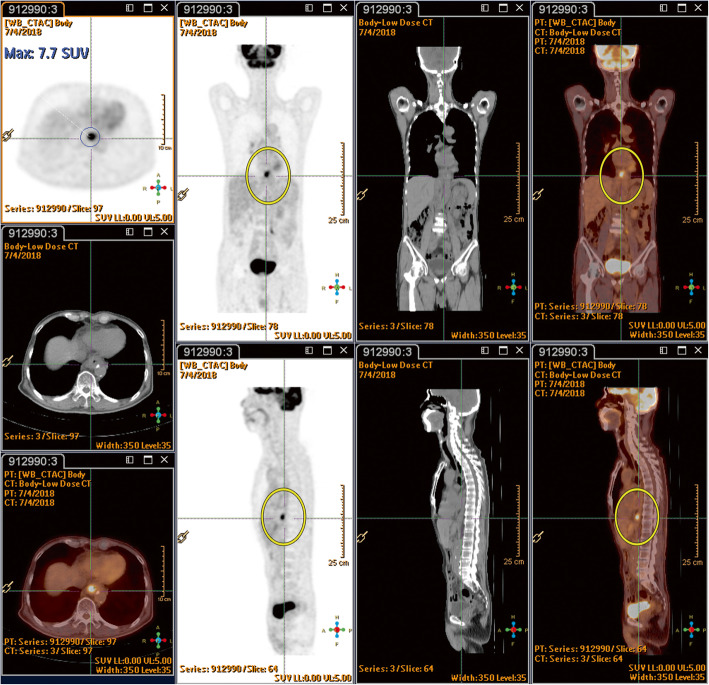
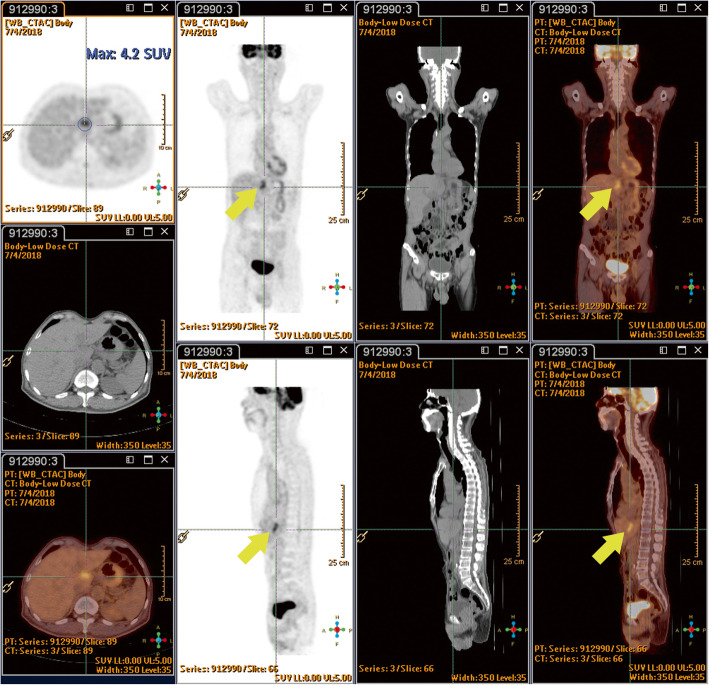
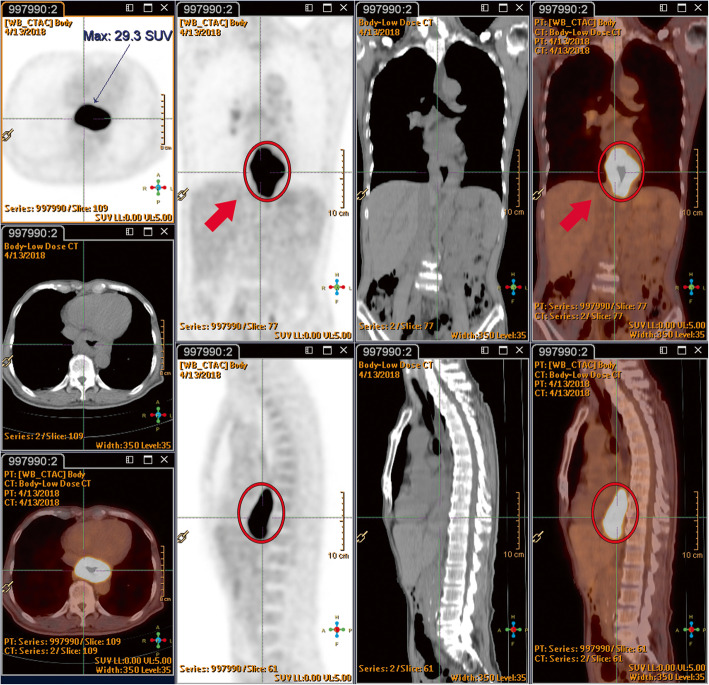
We report a case of a Asian male patient with distal esophageal cancer who had undergone neoadjuvant chemoradiotherapy (5000 cGy). Subsequently, a new lesion was discovered during a positron emission tomography with computed tomography scan 6 weeks later, near the left caudate lobe of the liver during tumor restaging. To exclude the possibility of liver metastasis, serial imaging was conducted, which included liver sonography, computed tomography, and magnetic resonance imaging for a more intimate probe. The patient's condition was verified as being liver inflammation change, as seen by the liver magnetic resonance imaging presentation. Thoracoscopic esophagectomy was performed with cervical esophagogastrostomy via the retrosternal route, along with a feeding jejunostomy. The procedure was performed smoothly, with an intraoperative liver biopsy also being conducted 2 weeks later, after positron emission tomography with computed tomography restaging. The pathology report revealed esophageal cancer in the form of poorly differentiated squamous cell carcinoma, pT3N1M0. The liver biopsy revealed obvious inflammation change after radiation therapy, which elucidated sinusoidal congestion with the attenuated hepatic cords and filled with erythrocytes. There was no evidence of liver metastasis. The patient recovered uneventfully and was discharged with his oral intake performing smoothly, and a stable condition was observed during 12 months of outpatient department follow-up.
New foci of increased F-fluorodeoxyglucose avidity are commonly seen in the caudate and left hepatic lobes of the liver during neoadjuvant chemoradiation for distal esophageal cancer, and these findings generally reflect radiation-induced liver disease rather than metastatic disease. Awareness of the pitfalls of a high F-fluorodeoxyglucose uptake in radiation-induced liver injury is crucial in order to avoid misinterpretation and overstaging. Except for the location of F-fluorodeoxyglucose uptake, the shape of the lesion, and an maximum standardized uptake value (> 10/h), a convincing liver magnetic resonance imaging scan or even a liver biopsy can provide accurate information for distinguishing radiotherapy-induced liver injury from liver metastasis.
新辅助放化疗目前是食管癌术前的金标准治疗方法。这种放射治疗有时会导致与食管病变平行的肝损伤,这类似于 F-氟脱氧葡萄糖正电子发射断层扫描与计算机断层扫描所显示的肝转移。在本报告中,我们发布了在手术过程中获得的虚拟放射诱导的肝损伤图像,以及相关的病理学,以便通过最佳决定性的影像学检查来确认假阳性结果。
我们报告了一名亚洲男性远端食管癌患者的病例,他接受了新辅助放化疗(5000cGy)。随后,在肿瘤重新分期的 6 周后,在肝脏左尾状叶附近的 F-氟脱氧葡萄糖正电子发射断层扫描与计算机断层扫描扫描中发现了一个新的病变。为了排除肝转移的可能性,进行了一系列的影像学检查,包括肝脏超声、计算机断层扫描和磁共振成像以进行更密切的探查。肝脏磁共振成像表现提示患者的病情为肝炎症改变,经确认。通过经胸骨后路径行颈胸段食管胃吻合术,同时行空肠造口术。手术过程顺利,2 周后在 F-氟脱氧葡萄糖正电子发射断层扫描与计算机断层扫描重新分期后进行了术中肝活检。病理报告显示为低分化鳞状细胞癌,pT3N1M0。肝活检显示放射治疗后明显的炎症改变,表现为窦状充血,肝索变细,充满红细胞。无肝转移证据。患者恢复顺利,出院后口服进食顺利,门诊随访 12 个月时情况稳定。
在新辅助放化疗治疗远端食管癌期间,肝脏的尾状叶和左叶通常会出现新的 F-氟脱氧葡萄糖摄取增加的焦点,这些发现通常反映的是放射性肝损伤而不是转移性疾病。了解放射性肝损伤中 F-氟脱氧葡萄糖摄取增加的陷阱对于避免误解和过度分期至关重要。除了 F-氟脱氧葡萄糖摄取的位置、病变的形状和最大标准化摄取值(>10/h)外,令人信服的肝脏磁共振成像扫描甚至肝活检可以提供准确的信息,用于区分放疗诱导的肝损伤与肝转移。