Seguro Fernanda Salles, Silva Carolina Maria Pinto Domingues Carvalho, Moura Carla Maria Boquimpani de, Conchon Monika, Fogliatto Laura, Funke Vaneuza Araujo Moreira, Abdo André, Macedo Ariane Vieira Scarlatelli, Santos Marilia Harumi Higushi Dos, Saraiva José Francisco Kerr
Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (HCFMUSP), São Paulo, SP, Brazil; Instituto do Câncer do Estado de São Paulo, (ICESPSP), São Paulo, SP, Brazil.
Instituto do Câncer do Estado de São Paulo, (ICESPSP), São Paulo, SP, Brazil; Universidade de São Paulo (USP), São Paulo, SP, Brazil.
Hematol Transfus Cell Ther. 2021 Apr-Jun;43(2):191-200. doi: 10.1016/j.htct.2020.04.009. Epub 2020 Jul 1.
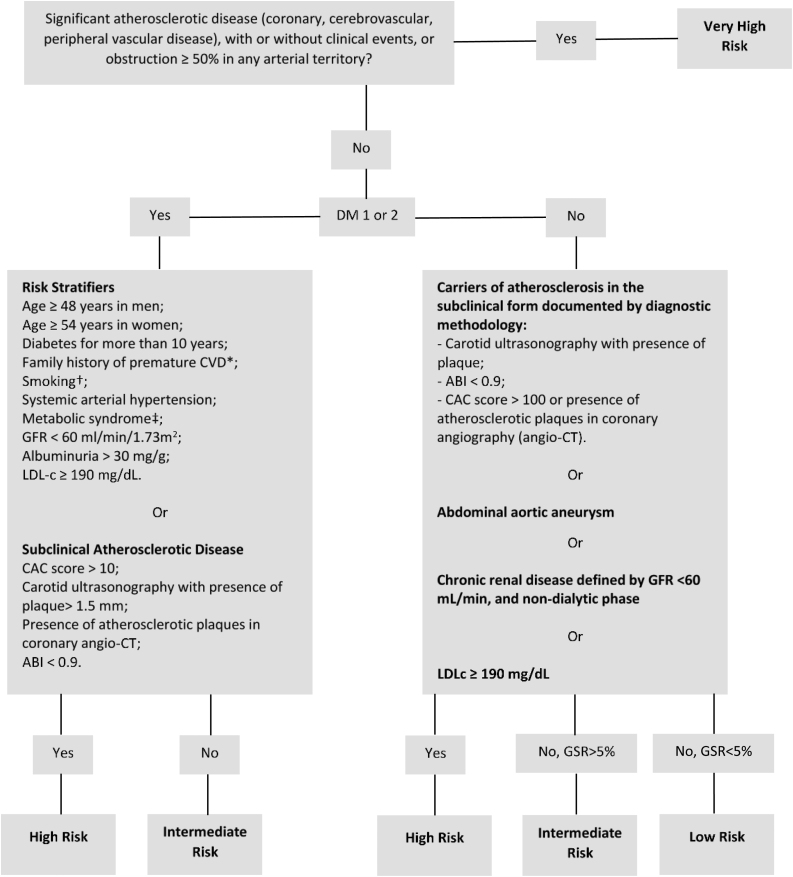
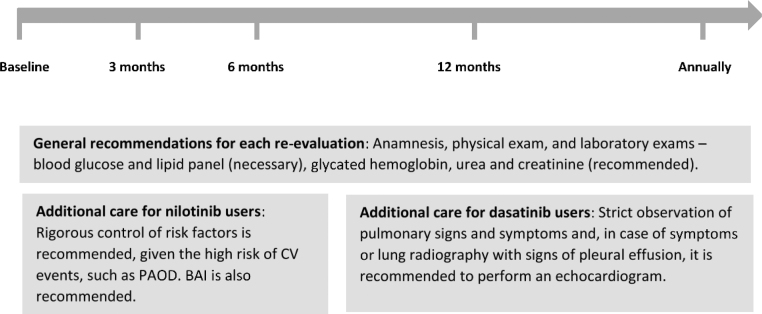
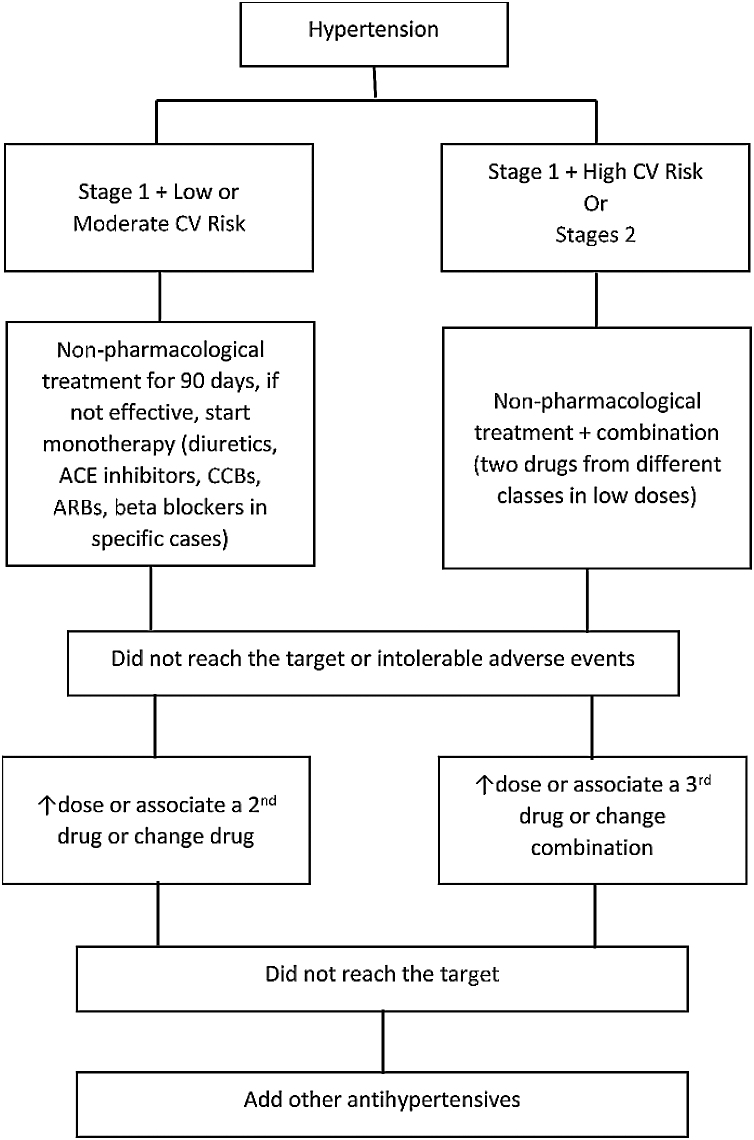
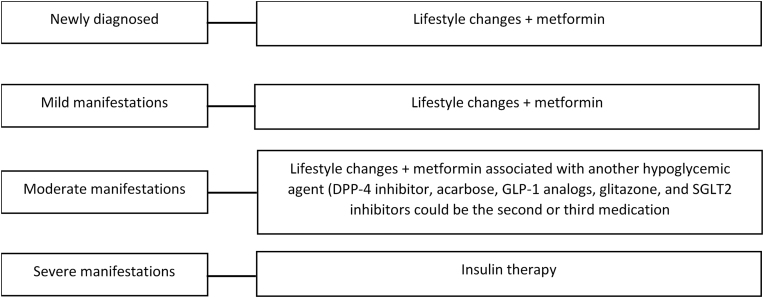
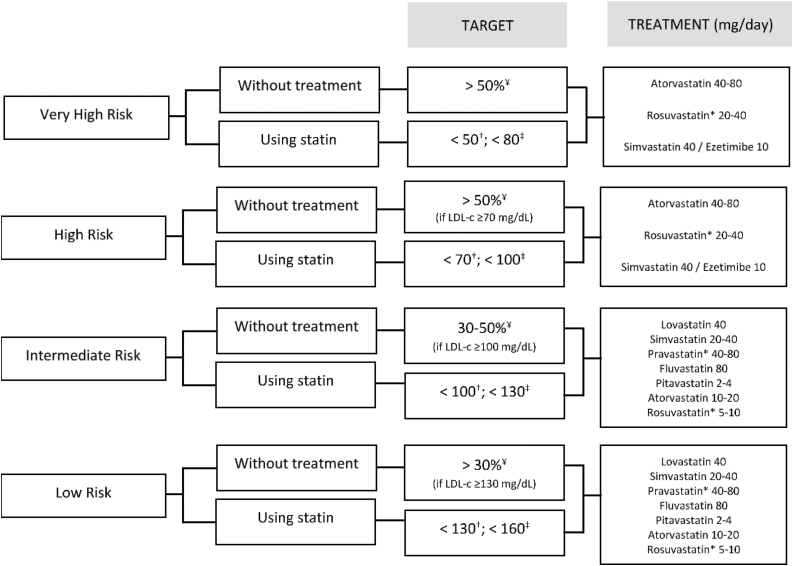
This manuscript summarizes the results of the consensus meeting composed of hematologists and cardiologists to establish recommendations for the prevention and follow-up of cardiovascular (CV) risk in patients with chronic myeloid leukemia (CML) treated with BCR-ABL tyrosine kinase inhibitors (TKIs) from the point of view of clinical practice and from the perspective of hematology consultation. In the first medical appointment, the CV risk factors should be identified to perform the baseline risk stratification, based on the Brazilian Guideline of Dyslipidemia and Atherosclerosis Prevention Update (risk levels: very high, high, intermediate and low). Once stratified, the treatment of the CV risk factors should be administered. If the patient presents risk factors, such as hypertension, diabetes, renal disease, smoking and hypercholesterolemia, the evaluation and initial treatment may be done by the hematologist, being an option the request for evaluation by a specialist. If the patient has a history of previous CV disease, we recommend referral to a specialist. As the CV risk score is dynamic and the control of risk factors can reduce the patient risk, this expert consensus recommends that the re-evaluation of the CV risk after the baseline should be performed at 3 months, 6 months and 12 months. After this period, it should be done annually and, for specific patients, at the clinician's discretion. The evaluation of the baseline CV risk and the safe administration of a TKI allow the patient to benefit from the maximum treatment, avoiding unwanted effects.
本手稿总结了血液科医生和心脏病专家组成的共识会议结果,从临床实践和血液学咨询角度,为接受BCR-ABL酪氨酸激酶抑制剂(TKIs)治疗的慢性髓性白血病(CML)患者的心血管(CV)风险预防和随访制定建议。在首次就诊时,应根据巴西血脂异常和动脉粥样硬化预防更新指南(风险水平:极高、高、中、低)识别CV风险因素,以进行基线风险分层。一旦分层,就应进行CV风险因素的治疗。如果患者存在高血压、糖尿病、肾病、吸烟和高胆固醇血症等风险因素,血液科医生可进行评估和初始治疗,也可选择请专科医生进行评估。如果患者有既往CV疾病史,我们建议转诊给专科医生。由于CV风险评分是动态的,控制风险因素可降低患者风险,本专家共识建议在基线后3个月、6个月和12个月进行CV风险重新评估。在此之后,应每年进行评估,对于特定患者,由临床医生酌情决定。基线CV风险评估和TKI的安全给药可使患者从最大程度的治疗中获益,避免不良影响。