Department of Neurosurgery, Stroke Center & Neurointervention, Chang Gung Memorial Hospital, Chang Gung Medical Center and University, 5, Fu-Shin Street, Kwei-Shan Hsiang, Taoyuan, 333, Taiwan.
Department of Neurosurgery, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, Guangdong, China.
BMC Neurol. 2020 Jul 7;20(1):271. doi: 10.1186/s12883-020-01856-4.
Cerebral vasospasm still results in high morbidity and mortality rates in patients after aneurysmal subarachnoid hemorrhage (SAH). The aim of this study was to establish a protocol for the management of vasospasm and demonstrate our experience of angioplasty using the Scepter XC balloon catheter.
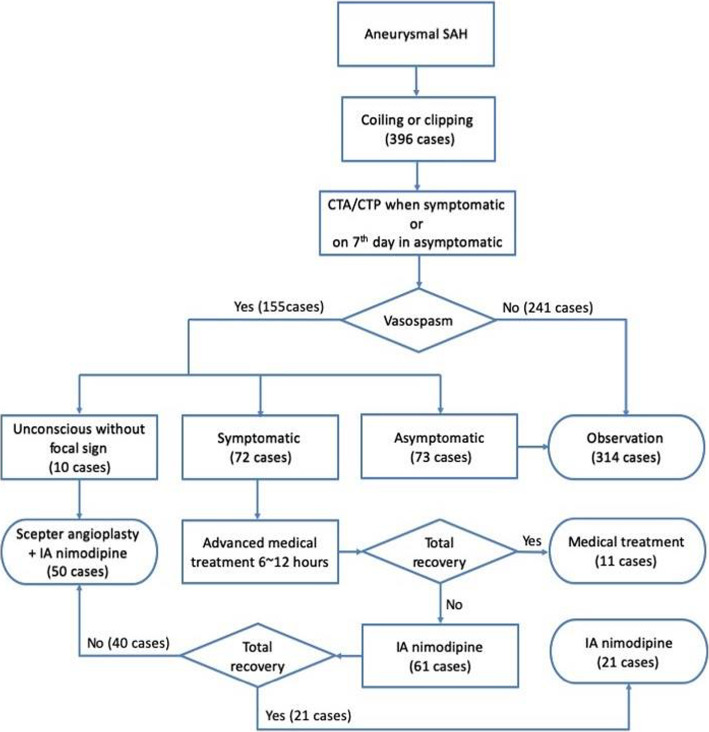
In this retrospective study, a computed tomography angiography and perfusion image was arranged if early symptoms occurred or on the 7th day following aneurysmal SAH. In patients with clear consciousness, balloon angioplasties were performed for symptomatic vasospasms, which were not improved within 6-12 h after maximal medical treatments. In unconscious patients, balloon angioplasties were performed for all patients with angiographic vasospasms.
Fifty patients underwent Scepter XC balloon angioplasty among 396 consecutive patients who accepted endovascular or surgical treatments for ruptured aneurysms. All angioplasty procedures were successful without complications. 100% angiographic improvement and 94% clinical improvement were reached immediately after the angioplasties. A favorable functional outcome (modified Rankin Score of ≤2) could be achieved in 82% of patients. Even in patients with poor clinical grading (Hunt-Hess grade 4-5), a clinical improvement rate of 87.5% and favorable outcome rate was 70.8% could be achieved.
Balloon angioplasty with Scepter XC balloon catheter is safe and effective for post-SAH vasospasm. This device's extra-compliant characteristics could considerably improve the quality of angioplasty procedures. For all patients, even those with poor neurological status, early treatment with combined protocol of nimodipine and angioplasty can have good clinical outcomes.
脑动脉痉挛仍然是蛛网膜下腔出血(SAH)患者高发病率和死亡率的原因。本研究旨在建立血管痉挛的管理方案,并展示我们使用 Scepter XC 球囊导管进行血管成形术的经验。
在这项回顾性研究中,如果早期出现症状或在 SAH 后第 7 天,安排进行计算机断层血管造影和灌注成像。对于有明确意识的患者,如果症状性血管痉挛在最大药物治疗后 6-12 小时内未得到改善,则进行球囊血管成形术。对于无意识的患者,所有血管造影显示血管痉挛的患者均进行球囊血管成形术。
在 396 例接受血管内或手术治疗破裂动脉瘤的连续患者中,有 50 例患者接受了 Scepter XC 球囊血管成形术。所有血管成形术均无并发症成功完成。血管成形术后即刻达到 100%的血管造影改善和 94%的临床改善。82%的患者可获得良好的功能结局(改良Rankin 评分≤2)。即使在临床分级较差的患者(Hunt-Hess 分级 4-5)中,也可达到 87.5%的临床改善率和 70.8%的良好结局率。
Scepter XC 球囊导管的血管成形术治疗 SAH 后血管痉挛是安全有效的。该设备的额外顺应性特征可显著提高血管成形术的质量。对于所有患者,即使是神经状态较差的患者,早期联合尼莫地平治疗和血管成形术可获得良好的临床结局。