Department of Neurology, Dokkyo Medical University, Tochigi, Japan.
Eli Lilly Japan K.K, Kobe, Japan.
BMC Neurol. 2020 Jul 8;20(1):274. doi: 10.1186/s12883-020-01848-4.
Real-world data on sufficient/insufficient response, and predictors of insufficient response, to acute treatments for migraine are limited in Japan. This study aimed to identify factors associated with insufficient response to acute treatment of migraine by exploring significant differences between people with migraine who sufficiently/insufficiently respond to prescribed acute treatment in Japan.
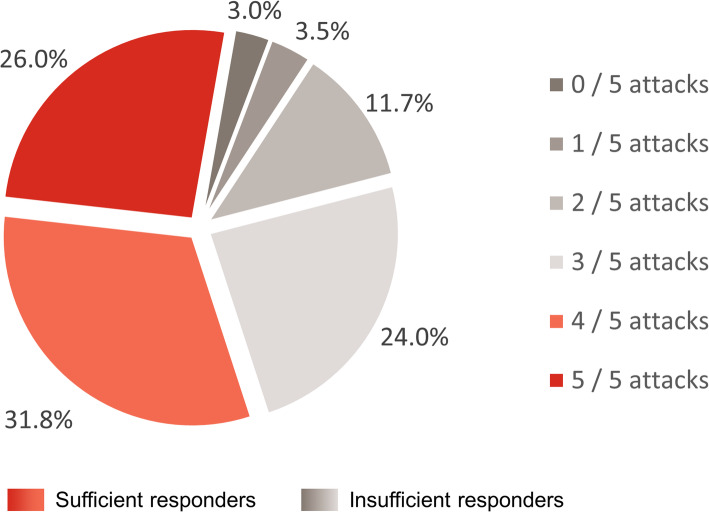
This was a retrospective analysis of 2014 Adelphi Migraine Disease Specific Programme cross-sectional survey data collected from physicians and their consulting adult patients with migraine in Japan. Insufficient responders to prescribed acute treatment were patients who achieved headache pain freedom within 2 h of acute treatment in no more than three of their last five migraine attacks. Factors associated with insufficient response to prescribed acute migraine treatment were identified using backward logistic regression.
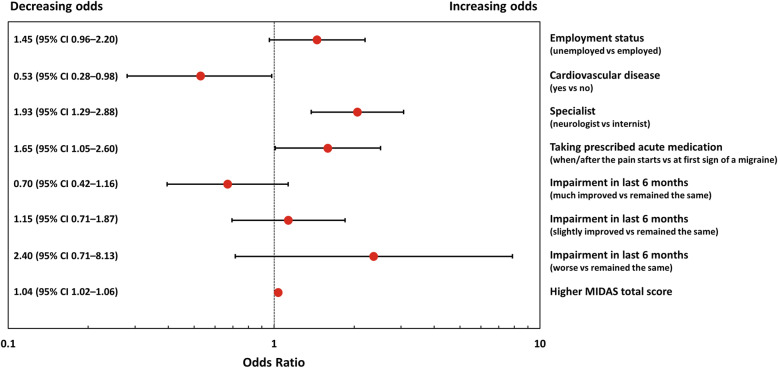
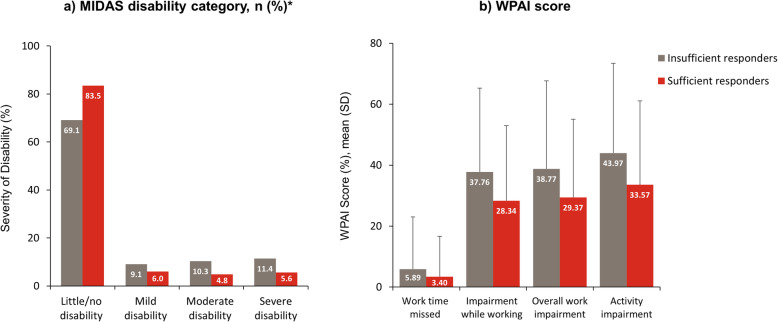
Overall, 227/538 (42.2%) patients were classified as insufficient responders to prescribed acute migraine treatment. Significantly more insufficient responders than sufficient responders had consulted a neurologist or a migraine/headache specialist, and had chronic migraine or medication-overuse or tension-type headaches (p < 0.05). More insufficient responders than sufficient responders reported taking acute treatment when/after the pain started (77.0 vs. 68.9%) than at first sign of migraine (p < 0.05). Compared with sufficient responders, insufficient responders reported a significantly higher mean ± standard deviation (SD) Migraine Disability Assessment total score (12.7 ± 23.3 vs. 5.8 ± 10.4, p < 0.001) and lower quality of life (EuroQol-5 Dimensions utility score 0.847 ± 0.19 vs. 0.883 ± 0.16, p = 0.024). Factors significantly associated with insufficient response to acute treatment included seeing a neurologist versus an internist (odds ratio [OR] 1.93; 95% confidence interval [CI] 1.29-2.88; p = 0.002), taking acute medication when/after pain started versus at first sign of migraine (OR 1.65; 95% CI 1.05-2.60; p = 0.030), a higher MIDAS total score (OR 1.04; 95% CI 1.02-1.06; p < 0.001), and presence of comorbid cardiovascular disease (OR 0.53; 95% CI 0.28-0.98; p = 0.044).
Many people with migraine in Japan struggle to adequately treat migraine attacks with prescribed acute medication and exhibit high levels of unmet need for acute treatment. Optimized management strategies utilizing existing therapeutic options as well as additional effective therapeutic options for migraine are required to improve symptoms and quality of life.
在日本,关于急性偏头痛治疗的充分/不充分反应以及不充分反应预测因素的真实世界数据有限。本研究旨在通过探讨日本偏头痛患者对急性治疗的充分/不充分反应之间的显著差异,确定与急性偏头痛治疗不充分反应相关的因素。
这是对 2014 年 Adelphi 偏头痛疾病专项计划的回顾性分析,该计划从日本的医生及其偏头痛成年患者中收集了横断面调查数据。急性治疗后不充分反应的患者是指在过去五次偏头痛发作中,急性治疗后 2 小时内头痛缓解至无疼痛的比例不超过三次的患者。使用向后逻辑回归识别与急性偏头痛治疗不充分反应相关的因素。
总体而言,538 例患者中有 227 例(42.2%)被归类为急性偏头痛治疗不充分反应者。与充分反应者相比,不充分反应者更多地咨询过神经科医生或偏头痛/头痛专家,并且患有慢性偏头痛或药物过度使用性头痛或紧张性头痛(p<0.05)。与充分反应者相比,更多的不充分反应者在疼痛开始时/之后(77.0%比 68.9%)而不是首次出现偏头痛时(p<0.05)服用急性治疗药物。与充分反应者相比,不充分反应者的偏头痛残疾评估总分(12.7±23.3 比 5.8±10.4,p<0.001)明显更高,生活质量(EuroQol-5 维度效用评分 0.847±0.19 比 0.883±0.16,p=0.024)更低。与急性治疗不充分反应显著相关的因素包括看神经科医生而非内科医生(比值比[OR]1.93;95%置信区间[CI]1.29-2.88;p=0.002),疼痛开始时/之后服用急性药物而非首次出现偏头痛时(OR 1.65;95%CI 1.05-2.60;p=0.030),MIDAS 总分较高(OR 1.04;95%CI 1.02-1.06;p<0.001),以及合并心血管疾病(OR 0.53;95%CI 0.28-0.98;p=0.044)。
许多日本偏头痛患者在使用处方急性药物治疗偏头痛发作时难以充分治疗,并且对急性治疗存在高度未满足的需求。需要优化管理策略,利用现有的治疗选择以及额外有效的偏头痛治疗选择,以改善症状和生活质量。