Division of Infectious Diseases & Hospital Epidemiology, University Hospital Basel, University Basel, Basel, Switzerland.
Division of Clinical Bacteriology and Mycology, University Hospital Basel, University Basel, Basel, Switzerland.
Euro Surveill. 2020 Jul;25(26). doi: 10.2807/1560-7917.ES.2020.25.26.1900317.
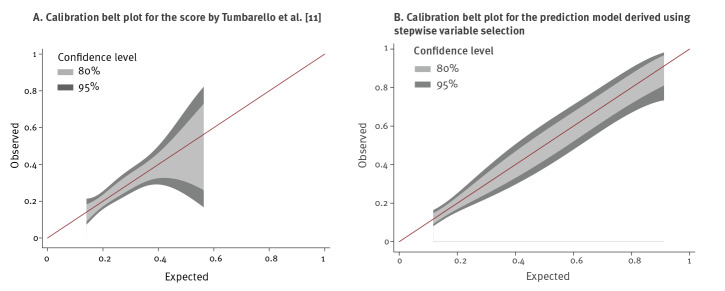
BackgroundAlgorithms for predicting infection with extended-spectrum β-lactamase-producing Enterobacterales (ESBL-PE) on hospital admission or in patients with bacteraemia have been proposed, aiming to optimise empiric treatment decisions.AimWe sought to confirm external validity and transferability of two published prediction models as well as their integral components.MethodsWe performed a retrospective case-control study at University Hospital Basel, Switzerland. Consecutive patients with ESBL-producing or isolated from blood samples between 1 January 2010 and 31 December 2016 were included. For each case, three non-ESBL-producing controls matching for date of detection and bacterial species were identified. The main outcome measure was the ability to accurately predict infection with ESBL-PE by measures of discrimination and calibration.ResultsOverall, 376 patients (94 patients, 282 controls) were analysed. Performance measures for prediction of ESBL-PE infection of both prediction models indicate adequate measures of calibration, but poor discrimination (area under receiver-operating curve: 0.627 and 0.651). History of ESBL-PE colonisation or infection was the single most predictive independent risk factor for ESBL-PE infection with high specificity (97%), low sensitivity (34%) and balanced positive and negative predictive values (80% and 82%).ConclusionsApplying published prediction models to institutions these were not derived from, may result in substantial misclassification of patients considered as being at risk, potentially leading to wrong allocation of antibiotic treatment, negatively affecting patient outcomes and overall resistance rates in the long term. Future prediction models need to address differences in local epidemiology by allowing for customisation according to different settings.
已经提出了用于预测医院入院或菌血症患者中产生超广谱β-内酰胺酶的肠杆菌科(ESBL-PE)感染的算法,旨在优化经验性治疗决策。
我们旨在确认两个已发表的预测模型及其组成部分的外部有效性和可转移性。
我们在瑞士巴塞尔大学医院进行了一项回顾性病例对照研究。纳入 2010 年 1 月 1 日至 2016 年 12 月 31 日期间从血液样本中分离出 ESBL 或 的连续患者。对于每个病例,确定了三个与检测日期和细菌种类相匹配的非 ESBL 产生对照。主要观察指标是通过区分和校准来准确预测 ESBL-PE 感染的能力。
总共分析了 376 例患者(94 例患者,282 例对照)。两种预测模型预测 ESBL-PE 感染的性能指标表明校准度适中,但区分度较差(接受者操作特征曲线下面积:0.627 和 0.651)。ESBL-PE 定植或感染史是 ESBL-PE 感染的最具预测性的独立危险因素,具有高特异性(97%)、低敏感性(34%)和平衡的阳性和阴性预测值(80%和 82%)。
将发表的预测模型应用于并非源自这些模型的机构可能会导致对被认为处于风险中的患者进行大量错误分类,这可能导致抗生素治疗分配不当,从而对患者结局和长期整体耐药率产生负面影响。未来的预测模型需要通过允许根据不同环境进行定制来解决当地流行病学的差异。