Cheng Yumei, Yuan Jia, Chen Qimin, Shen Feng
Department of Critical Care Medicine, The Affiliated Hospital of Guizhou Medical University, Guizhou 550001, China.
Ann Transl Med. 2020 Jun;8(12):758. doi: 10.21037/atm-20-4171.
The Department of Critical Care Medicine has the highest risk of nosocomial infection. This study used an autoregressive integrated moving average (ARIMA) model to simulate the prevalence of nosocomial infections in the Department of Critical Care Medicine of Guizhou Province. We also provided a policy basis for the prevention and control of hospital infection in the Department of Critical Care Medicine of Guizhou Province.
The data of ventilator-associated pneumonia, vascular catheter-related bloodstream infections, and urinary tract intubation-related urinary tract infections in nine tertiary A comprehensive treatment hospitals in Guizhou province from January 2014 to December 2019 were collected. The ARIMA time series model was used to evaluate the model fitting and prediction effects.
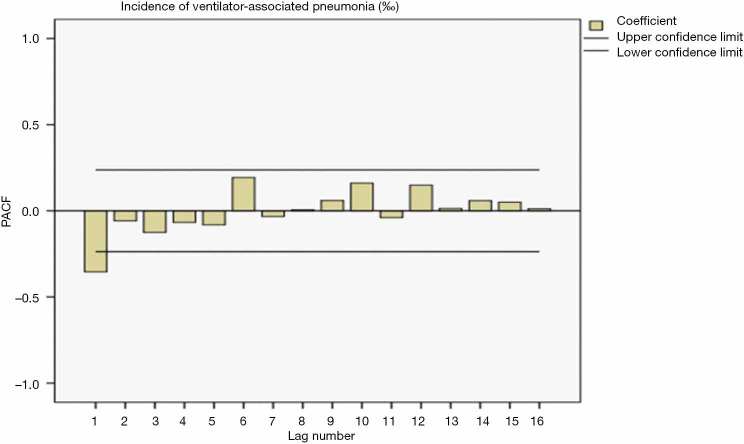
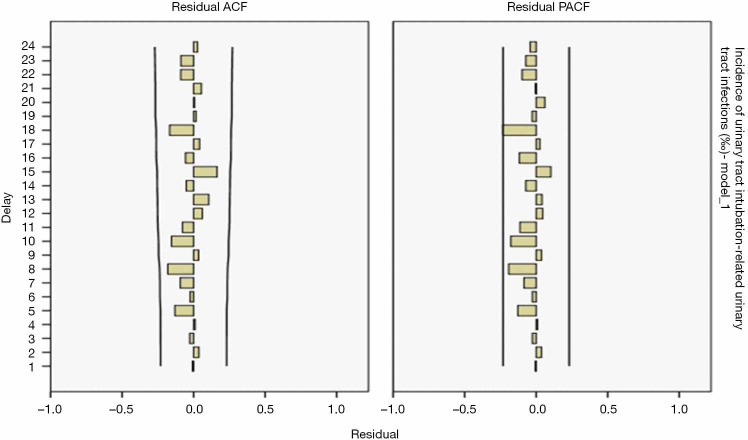
After comparison, in the Department of Critical Care Medicine of Guizhou Province, the unsurpassed model of ventilator-associated pneumonia was the ARIMA (0,1,1) model, with a residual Ljuing-Box Q test result of Q=10.832 (P=0.865), suggesting it is a white noise sequence and its simulation and prediction effects are beneficial. The best model of vascular catheter-related bloodstream infection was the ARIMA (0,0,1) model, with a residual Ljuing-Box Q test result of Q=14.914 (P=0.602). These results suggest that it is a white noise sequence, and its simulation and prediction effects are sufficient. The optimal model of urinary tract intubation-related urinary tract infection is ARIMA (1,0,0), and the residual Ljuing-Box Q test result is Q=15.042 (P=0.592), suggesting it is a white noise sequence with an accurate simulation and prediction effect.
The ARIMA model can accurately simulate and predict nosocomial infection incidence rate in the Department of Critical Care Medicine of Guizhou Province, and can provide a reference for the prevention and control of nosocomial infections.
重症医学科医院感染风险最高。本研究采用自回归积分滑动平均(ARIMA)模型模拟贵州省重症医学科医院感染的流行情况。我们还为贵州省重症医学科医院感染的预防与控制提供了政策依据。
收集贵州省9家三级甲等综合医院2014年1月至2019年12月呼吸机相关性肺炎、血管导管相关血流感染和导尿管相关尿路感染的数据。采用ARIMA时间序列模型评估模型拟合和预测效果。
经比较,在贵州省重症医学科,呼吸机相关性肺炎的最优模型为ARIMA(0,1,1)模型,残差Ljung-Box Q检验结果为Q = 10.832(P = 0.865),表明其为白噪声序列,模拟和预测效果良好。血管导管相关血流感染的最佳模型为ARIMA(0,0,1)模型,残差Ljung-Box Q检验结果为Q = 14.914(P = 0.602)。这些结果表明其为白噪声序列,模拟和预测效果充分。导尿管相关尿路感染的最优模型为ARIMA(1,0,0),残差Ljung-Box Q检验结果为Q = 15.042(P = 0.592),表明其为白噪声序列,模拟和预测效果准确。
ARIMA模型能够准确模拟和预测贵州省重症医学科医院感染发病率,可为医院感染的预防与控制提供参考。