German Center for Vertigo and Balance Disorders (DSGZ), Ludwig-Maximilians University of Munich, Klinikum Grosshadern, Marchioninistrasse 15, 81377, Munich, Germany.
Department of Neurology, Schoen Clinic Bad Aibling, Bad Aibling, Germany.
J Neurol. 2020 Dec;267(Suppl 1):118-125. doi: 10.1007/s00415-020-10019-x. Epub 2020 Jul 11.
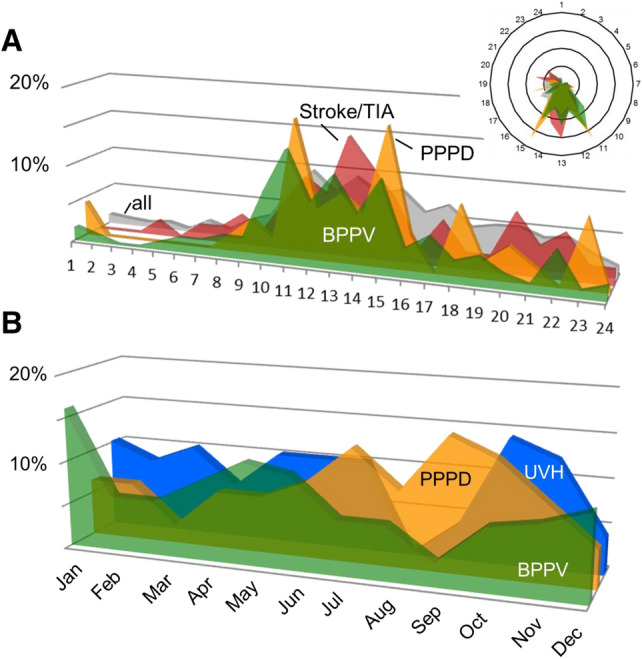
Distinguishing between serious (e.g., stroke) and benign (e.g., benign paroxysmal positional vertigo, BPPV) disorders remains challenging in emergency consultations for vertigo and dizziness (VD). A number of clues from patient history and clinical examination, including several diagnostic index tests have been reported recently. The objective of the present study was to analyze frequency and distribution patterns of specific vestibular and non-vestibular diagnoses in an interdisciplinary university emergency room (ER), including data on daytime and season of presentation. A retrospective chart analysis of all patients seen in a one-year period was performed. In the ER 4.23% of all patients presented with VD (818 out of 19,345). The most frequent-specific diagnoses were BPPV (19.9%), stroke/transient ischemic attack (12.5%), acute unilateral vestibulopathy/vestibular neuritis (UVH; 8.3%), and functional VD (8.3%). Irrespective of the diagnosis, the majority of patients presented to the ER between 8 a.m. and 4 p.m. There are, however, seasonal differences. BPPV was most prevalent in December/January and rare in September. UVH was most often seen in October/November; absolute and relative numbers were lowest in August. Finally, functional/psychogenic VD was common in summer and autumn with highest numbers in September/October and lowest numbers in March. In summary, daytime of presentation did not distinguish between diagnoses as most patients presented during normal working hours. Seasonal presentation revealed interesting fluctuations. The UVH peak in autumn supports the viral origin of the condition (vestibular neuritis). The BPPV peak in winter might be related to reduced physical activity and low vitamin D. However, it is likely that multiple factors contribute to the fluctuations that have to be disentangled in further studies.
在眩晕和头晕(VD)的急诊咨询中,区分严重(例如中风)和良性(例如良性阵发性位置性眩晕,BPPV)疾病仍然具有挑战性。最近报道了一些来自病史和临床检查的线索,包括几种诊断性指数测试。本研究的目的是分析在跨学科大学急诊室(ER)中特定前庭和非前庭诊断的频率和分布模式,包括呈现的日间和季节数据。对一年期间所有就诊患者的回顾性图表分析。在 ER 中,所有患者中有 4.23%(19,345 例中有 818 例)出现 VD。最常见的特定诊断是 BPPV(19.9%)、中风/短暂性脑缺血发作(12.5%)、急性单侧前庭病/前庭神经炎(UVH;8.3%)和功能性 VD(8.3%)。无论诊断如何,大多数患者在上午 8 点至下午 4 点之间到 ER 就诊。但是,存在季节性差异。BPPV 在 12 月/1 月最常见,在 9 月很少见。UVH 最常见于 10 月/11 月;8 月的绝对和相对数量最低。最后,功能性/心因性 VD 在夏季和秋季很常见,9 月/10 月数量最多,3 月数量最少。总之,就诊的白天并不能区分诊断,因为大多数患者在正常工作时间就诊。季节呈现出有趣的波动。秋季 UVH 高峰支持该疾病的病毒起源(前庭神经炎)。冬季 BPPV 高峰可能与体力活动减少和维生素 D 水平低有关。然而,可能有多种因素导致波动,需要在进一步的研究中加以阐明。