Li Ye, Zhang Zhibo, Hu Yi, Yan Xiang, Song Qi, Wang Guoqiang, Chen Runzhe, Jiao Shunchang, Wang Jinliang
Department of Oncology, The First Medical Center of Chinese PLA General Hospital, Beijing, China.
Oncology Laboratory, The First Medical Center of Chinese PLA General Hospital, Beijing, China.
Front Oncol. 2020 Jun 23;10:654. doi: 10.3389/fonc.2020.00654. eCollection 2020.
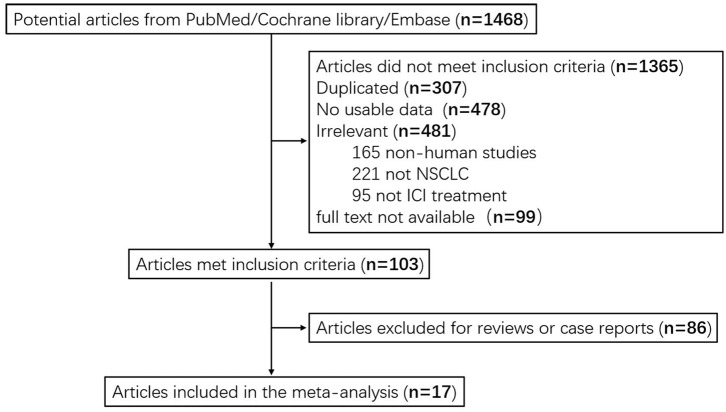
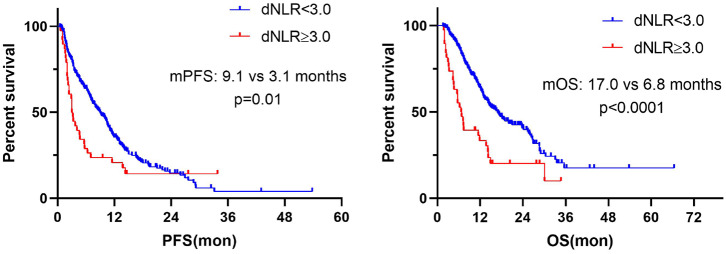
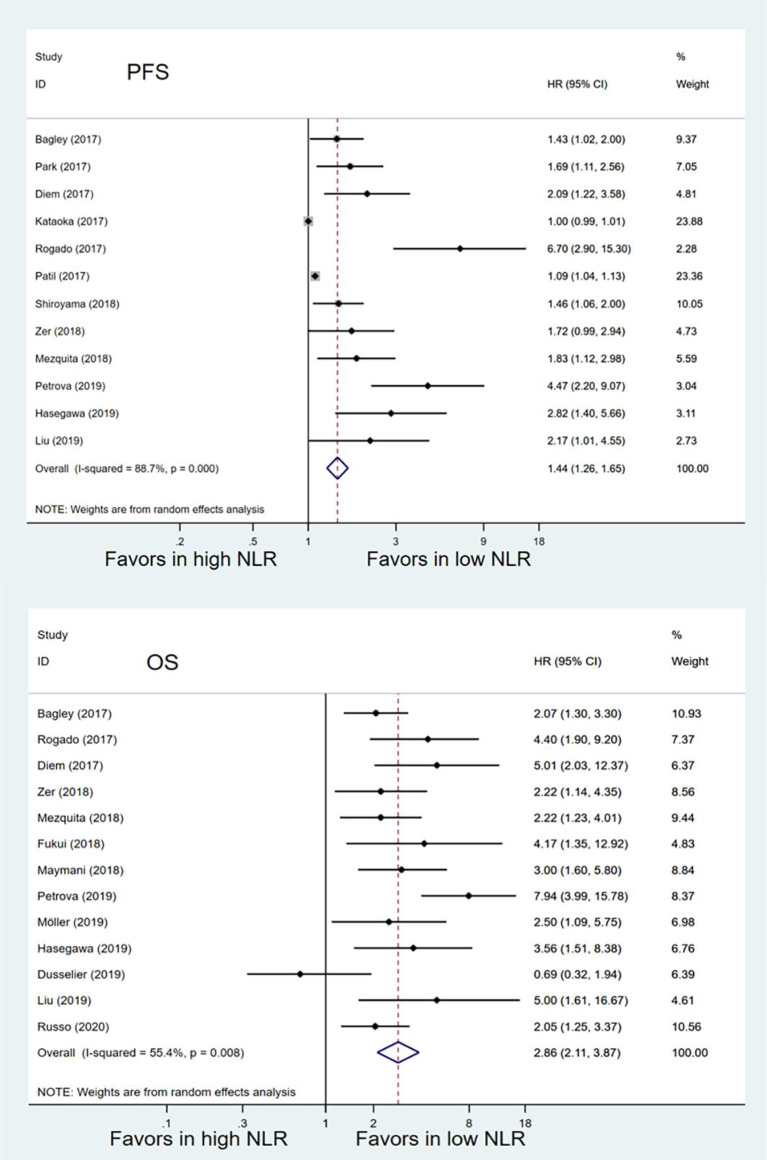
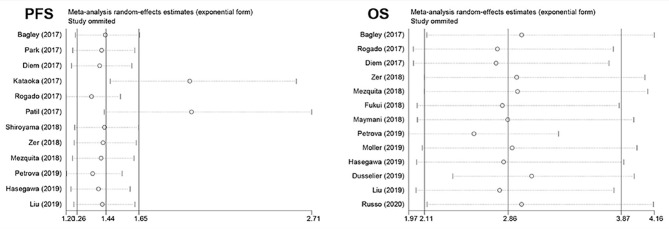
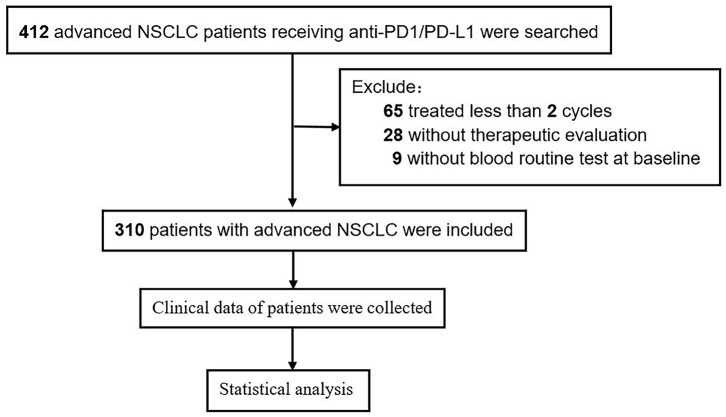
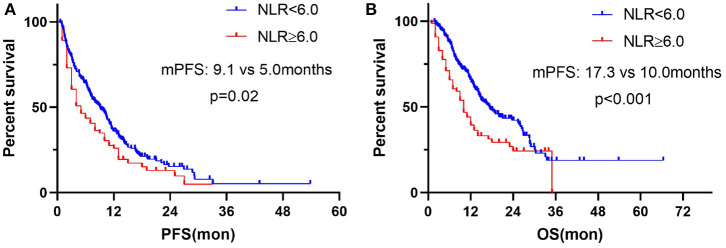
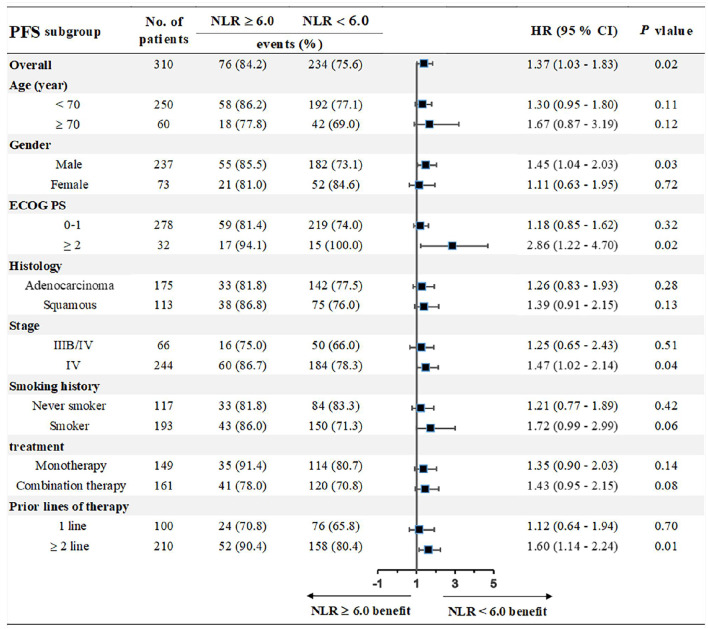
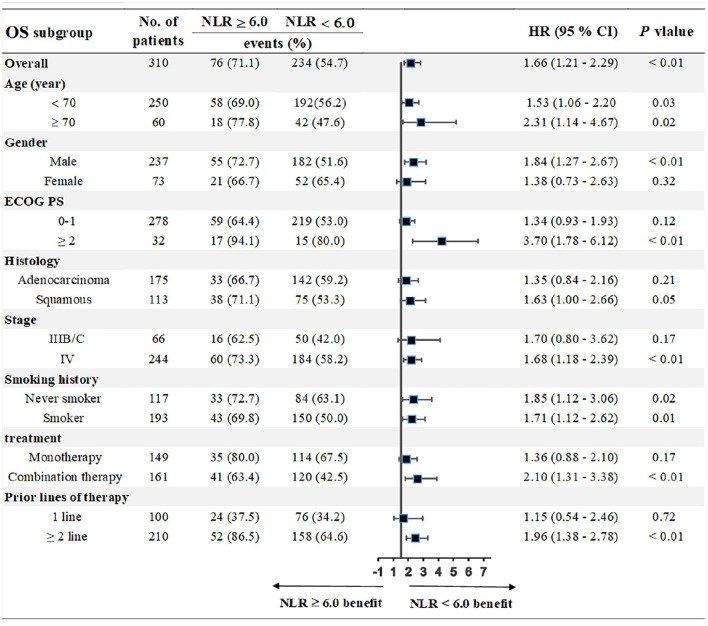
Recent studies have demonstrated the predictive value of pretreatment neutrophil-to-lymphocyte ratio (NLR) in advanced cancers; however, the role of NLR in patients with advanced non-small-cell lung cancer (NSCLC) treated with immune checkpoint inhibitors (ICIs) remained to be explored. Thus, we aimed to investigate whether pretreatment NLR was associated with the outcomes of advanced NSCLC patients treated with ICIs. A comprehensive literature research was first conducted in PubMed, the Cochrane Central Library, and Embase for studies that evaluated the association between pretreatment NLR and survival of advanced NSCLC patients with ICIs treatment. We then conducted a retrospective study in Chinese People's Liberation Army (PLA) General Hospital (Beijing, China) to validate these findings. A total of 17 eligible studies with 2,106 patients were included in our meta-analysis, of which, 12 studies reported progression-free survival (PFS), and 13 studies reported overall survival (OS). The pooled results showed that high pretreatment NLR was significantly associated with poorer PFS (HR = 1.44, 95% CI 1.26-1.65; < 0.001) and OS (HR = 2.86, 95% CI 2.11-3.87; < 0.001) compared with those with low pretreatment NLR. Subgroup analysis demonstrated that the association between baseline NLR and PFS remained significant except that the cut-off value of NLR was 3 (HR = 1.48, 95% CI 0.93-2.37; = 0.098) and region of Asia (HR = 1.55, 95% CI 1.00-2.39; = 0.051). These results were further validated in our retrospective study that patients with pretreatment NLR ≥ 6.0 had shorter PFS (median: 5.0 vs. 9.1 months, HR = 1.39; 95% CI 1.01-1.91; = 0.02) and OS (median: 10.0 vs. 17.3 months, HR = 1.71; 95% CI 1.18-2.46; < 0.001) compared with those with NLR < 6.0. The associations between NLR and survival were consistent in subgroup analysis stratified by age, gender, ECOG PS, histology, stage, smoking history, treatment, and prior lines of therapy. Dynamics of NLR (dNLR) that increased ≥3.0 from baseline was also significantly associated with worse PFS (median: 3.1 vs. 9.1 months; = 0.01) and OS (median: 6.8 vs. 17.0 months; < 0.0001). Our study demonstrates that pretreatment NLR and dNLR from baseline are associated with the outcomes of advanced NSCLC patients treated with ICIs; however, it warrants further prospective studies.
近期研究已证实治疗前中性粒细胞与淋巴细胞比值(NLR)在晚期癌症中的预测价值;然而,NLR在接受免疫检查点抑制剂(ICI)治疗的晚期非小细胞肺癌(NSCLC)患者中的作用仍有待探索。因此,我们旨在研究治疗前NLR是否与接受ICI治疗的晚期NSCLC患者的预后相关。首先在PubMed、Cochrane中心图书馆和Embase中进行了全面的文献检索,以查找评估治疗前NLR与接受ICI治疗的晚期NSCLC患者生存率之间关联的研究。然后我们在中国人民解放军总医院(北京,中国)进行了一项回顾性研究以验证这些发现。我们的荟萃分析共纳入了17项符合条件的研究,涉及2106例患者,其中12项研究报告了无进展生存期(PFS),13项研究报告了总生存期(OS)。汇总结果显示,与治疗前NLR较低的患者相比,治疗前NLR较高与较差的PFS(HR = 1.44,95%CI 1.26 - 1.65;P < 0.001)和OS(HR = 2.86,95%CI 2.11 - 3.87;P < 0.001)显著相关。亚组分析表明,除了NLR的临界值为3(HR = 1.48,95%CI 0.93 - 2.37;P = 0.098)和亚洲地区(HR = 1.55,95%CI 1.00 - 2.39;P = 0.051)外,基线NLR与PFS之间的关联仍然显著。这些结果在我们的回顾性研究中得到进一步验证,即治疗前NLR≥6.0的患者与NLR < 6.0的患者相比,PFS更短(中位数:5.0 vs. 9.1个月,HR = 1.39;95%CI 1.01 - 1.91;P = 0.02),OS也更短(中位数:10.0 vs. 17.3个月,HR = 1.71;95%CI 1.18 - 2.46;P < 0.001)。在按年龄、性别、东部肿瘤协作组(ECOG)体能状态、组织学类型、分期、吸烟史、治疗和既往治疗线数分层的亚组分析中,NLR与生存率之间的关联是一致的。治疗前NLR从基线升高≥3.0的NLR动态变化(dNLR)也与较差的PFS(中位数:3.1 vs. 9.1个月;P = 0.01)和OS(中位数:6.8 vs. 17.0个月;P < 0.0001)显著相关。我们的研究表明,治疗前NLR和基线dNLR与接受ICI治疗的晚期NSCLC患者的预后相关;然而,这需要进一步的前瞻性研究。