WHO Collaborating Centre for Public Health aspects of musculo-skeletal health and aging, Division of Public Health, Epidemiology and Health Economics, University of Liège, Liège, Belgium.
Geriatrics Department, Parc de Salut Mar, Barcelona, Spain.
J Cachexia Sarcopenia Muscle. 2020 Oct;11(5):1200-1211. doi: 10.1002/jcsm.12574. Epub 2020 Jul 13.
The Global Leadership Initiative on Malnutrition (GLIM) criteria have been recently launched by consensus of the major nutrition societies. GLIM criteria are partly constructed on the previous definition of malnutrition developed by the European Society of Clinical Nutrition and Metabolism (ESPEN). We aimed to assess malnutrition according to the ESPEN and GLIM criteria at baseline and to determine the corresponding risk of mortality during a 4-year follow-up in community-dwelling older adults from the SarcoPhAge (Sarcopenia and Physical Impairment with advancing Age) study. The relationship between malnutrition and incidence of 4-year adverse health consequences (institutionalization, hospitalization, falls, and fractures) was assessed.
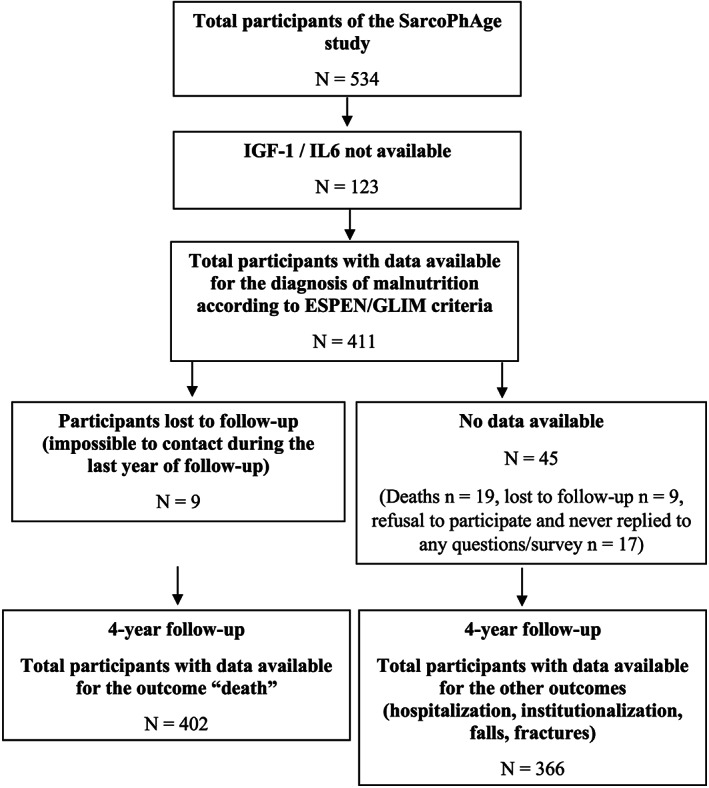
This prospective population-based cohort was part of SarcoPhAge, which included 534 older adults in Belgium, followed up from 2013 to 2019. Community-dwelling healthy volunteers ≥65 years old were recruited. Mortality and adverse health consequences were collected annually by interview or phone call. Baseline malnutrition was defined according to the GLIM and ESPEN criteria. Agreement between the two definitions was reported by Cohen's kappa coefficient. Adjusted Cox regression and Kaplan-Meier survival curves were performed for malnutrition. Logistic regression was used for the other outcomes.
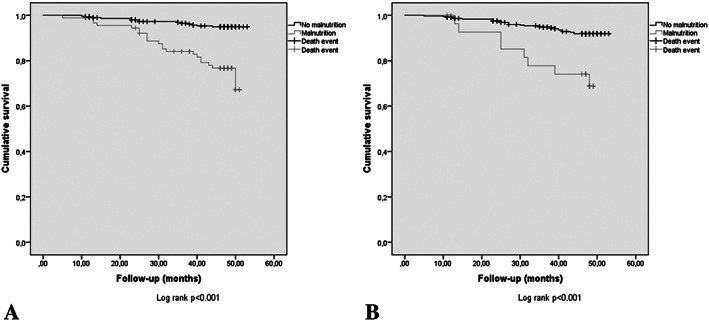
From 534 subjects in SarcoPhAge, the records for 411 participants (73.2 ± 6.05 years old; 55.7% women) had all the variables needed to apply the GLIM criteria. Prevalence of baseline malnutrition was 23.4% for GLIM and 7% for ESPEN criteria (k = 0.30, low agreement). The adjusted Cox regression showed a significant increased mortality risk according to malnutrition status as defined by the GLIM [adjusted hazard ratio = 4.41 (95% confidence interval: 2.17-8.97)] and ESPEN [adjusted hazard ratio = 2.76 (95% confidence interval: 1.16-6.58)] criteria. Survival curves differed significantly between malnourished and non-malnourished groups, regardless of the definition used (log rank P < 0.001 for both). No association was found between baseline malnutrition according to these two criteria and 4-year risk of institutionalization, hospitalization, falls, or fractures (all P > 0.05).
Malnutrition according to the GLIM criteria was associated with a 4.4-fold higher mortality risk, double that of the ESPEN criteria, during a 4-year follow-up. No association was found between malnutrition according to these two criteria and incidence of other health adverse consequences. GLIM criteria anticipate mortality and might guide interventions, with important implications for clinical practice and research.
全球营养不良领导倡议 (GLIM) 标准最近已由主要营养学会达成共识推出。GLIM 标准部分基于欧洲临床营养与代谢学会 (ESPEN) 之前制定的营养不良定义。我们旨在根据 ESPEN 和 GLIM 标准评估 SarcoPhAge(肌肉减少症和身体机能障碍与年龄增长)研究中社区居住的老年人基线时的营养不良情况,并确定 4 年随访期间的相应死亡率。评估了营养不良与 4 年不良健康后果(住院、住院、跌倒和骨折)发生率之间的关系。
这项前瞻性基于人群的队列研究是 SarcoPhAge 的一部分,该研究包括 534 名比利时社区居住的老年人,随访时间为 2013 年至 2019 年。招募了≥65 岁的健康志愿者。通过面谈或电话每年收集死亡率和不良健康后果。根据 GLIM 和 ESPEN 标准定义基线营养不良。报告两种定义之间的一致性采用 Cohen's kappa 系数。对营养不良进行调整后的 Cox 回归和 Kaplan-Meier 生存曲线。使用逻辑回归评估其他结局。
在 SarcoPhAge 的 534 名受试者中,有 411 名参与者(73.2±6.05 岁;55.7%为女性)的记录包含应用 GLIM 标准所需的所有变量。根据 GLIM 标准,基线时营养不良的患病率为 23.4%,根据 ESPEN 标准为 7%(k=0.30,一致性低)。调整后的 Cox 回归显示,根据 GLIM 定义的营养不良状态,死亡率风险显著增加[调整后的危险比=4.41(95%置信区间:2.17-8.97)]和 ESPEN [调整后的危险比=2.76(95%置信区间:1.16-6.58)]标准。无论使用哪种定义,营养不良组和非营养不良组的生存曲线差异均有统计学意义(log rank P<0.001,均)。根据这两个标准,基线营养不良与 4 年住院、住院、跌倒或骨折风险之间没有关联(均 P>0.05)。
根据 GLIM 标准的营养不良与 4 年随访期间 4.4 倍的死亡率风险相关,是 ESPEN 标准的两倍。根据这两个标准的营养不良与其他健康不良后果的发生率之间没有关联。GLIM 标准可以预测死亡率,并可能指导干预措施,对临床实践和研究具有重要意义。