Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden
Department of Medicine Solna, Karolinska Institutet, Stockholm, Sweden.
RMD Open. 2020 Jul;6(2). doi: 10.1136/rmdopen-2020-001201.
To compare incidence rates of gastrointestinal (GI) perforations between patients with RA and the general population, and between patients treated with tumour necrosis factor inhibitors (TNFi) and non-TNFi biologics.
In this nationwide cohort study, a total of 63 532 patients with RA, with 26 050 biological treatment episodes (TNFi, rituximab, abatacept or tocilizumab) and 76 304 general population controls, were followed between 2009 and 2017 until the first outcome event. The main outcome was hospitalisation or death due to lower GI perforations, identified according to a prespecified list of ICD-10 (International Classification of Diseases, 10th revision) codes. Inverse probability of treatment weighting was used for adjustment.
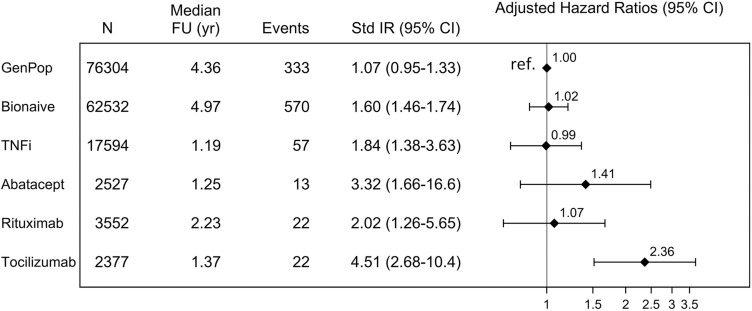
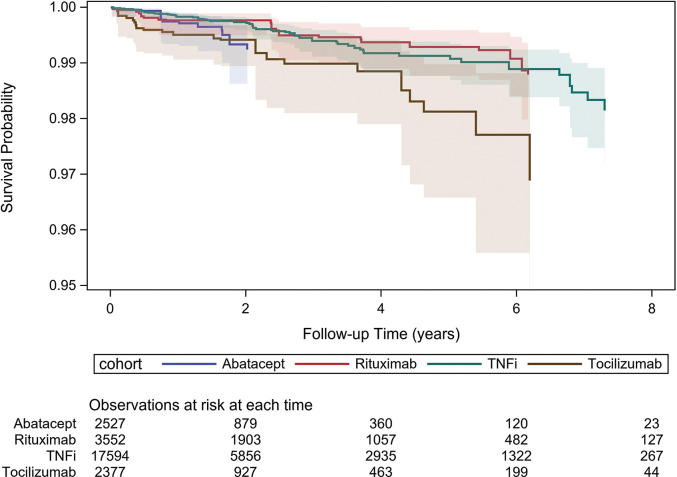
The sex-standardised and age-standardised incidence rates of lower GI perforations were 1.1 (95% CI 1.0 to 1.3) events per 1000 person-years among general population controls, 1.6 (1.5-1.7) among bionaïve patients and ranged from 1.8 (1.4-3.6) (TNFi) to 4.5 (2.7-10.4) (tocilizumab) among biologics-treated patients. After adjustment for glucocorticoid use, the risk in bionaïve, TNFi-treated, abatacept-treated or rituximab-treated patients with RA was no longer different from the general population, while for tocilizumab it remained significantly higher. Comparing tocilizumab to TNFi, the adjusted HR for lower GI perforations was 2.2 (1.3-3.8), corresponding to one additional GI perforation per 451 patient-years treated with tocilizumab instead of TNFi.
Tocilizumab was associated with a higher risk of lower GI perforations compared with alternative biologics. In absolute numbers, the risk remained low on all biologics commonly used to treat RA, but the accumulated evidence across settings and outcome definitions supports that this risk should be considered in treatment guidelines for RA.
比较类风湿关节炎(RA)患者与普通人群、肿瘤坏死因子抑制剂(TNFi)与非 TNFi 生物制剂治疗患者胃肠道(GI)穿孔的发生率。
在这项全国性队列研究中,共纳入 63532 例 RA 患者,其中 26050 例接受生物治疗(TNFi、利妥昔单抗、阿巴西普或托珠单抗),76304 例为普通人群对照,于 2009 年至 2017 年期间进行随访,直至首次发生结局事件。主要结局为下 GI 穿孔导致的住院或死亡,根据 ICD-10(国际疾病分类,第 10 版)代码预先指定的清单进行确定。采用逆概率治疗加权法进行调整。
普通人群对照的下 GI 穿孔标准化性别发病率和标准化年龄发病率为 1.1(95%CI,1.0 至 1.3)/1000 人年,生物制剂初治患者为 1.6(1.5 至 1.7),生物制剂治疗患者的发病率范围为 1.8(1.4 至 3.6)(TNFi)至 4.5(2.7 至 10.4)(托珠单抗)。调整糖皮质激素使用后,RA 患者中生物制剂初治、TNFi 治疗、阿巴西普治疗或利妥昔单抗治疗患者的风险与普通人群无差异,而托珠单抗仍显著更高。与 TNFi 相比,托珠单抗治疗下 GI 穿孔的调整后 HR 为 2.2(1.3 至 3.8),即每 451 例接受托珠单抗治疗而非 TNFi 治疗的患者中,就会发生 1 例额外的 GI 穿孔。
与其他生物制剂相比,托珠单抗与下 GI 穿孔风险增加相关。在所有常用的 RA 治疗生物制剂中,绝对风险仍然较低,但在不同环境和结局定义下的累积证据支持在 RA 治疗指南中考虑这种风险。