Abhilash K P, Acharya H, Dua J, Kumar S, Selvaraj B, Priya G
Department of Emergency Medicine, Christian Medical College, Vellore, Tamil Nadu, India.
J Postgrad Med. 2020 Jul-Sep;66(3):128-132. doi: 10.4103/jpgm.JPGM_637_19.
Although oxygen is one of the oldest drugs available, it is still one of the most inappropriately administered drugs leading to over utilization of this very expensive resource.
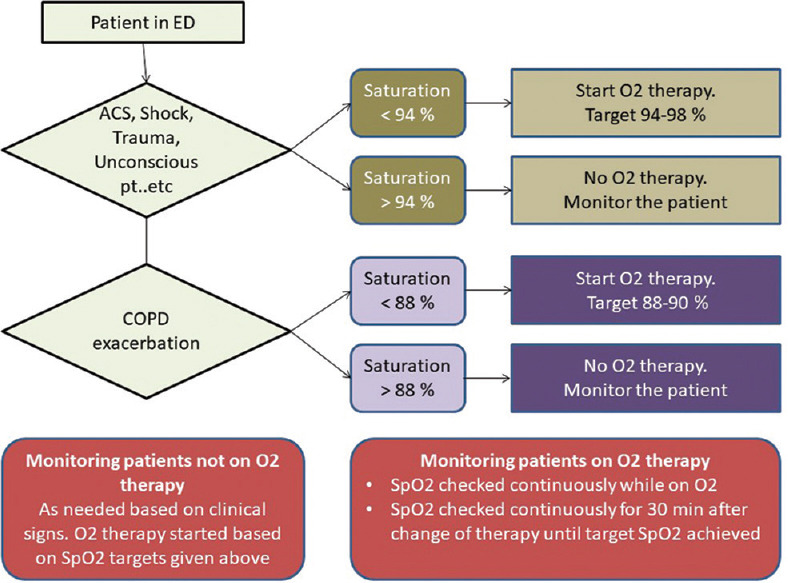
This prospective observational study was done in a large emergency department (ED) in India. The pattern of oxygen usage was studied before and after the strict implementation of an oxygen treatment algorithm. The algorithm was taught to all doctors and nurses and its implementation was monitored regularly. The main outcome measures were proportion of patients receiving oxygen therapy, inappropriate usage, and avoidable direct medical cost to the patient.
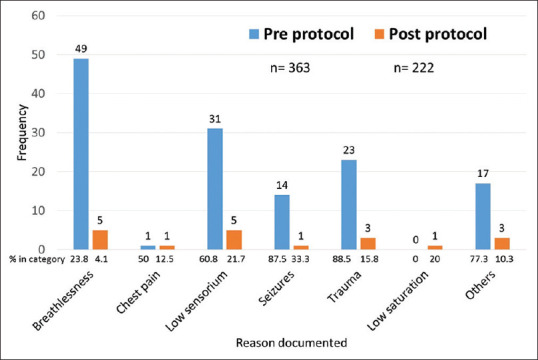
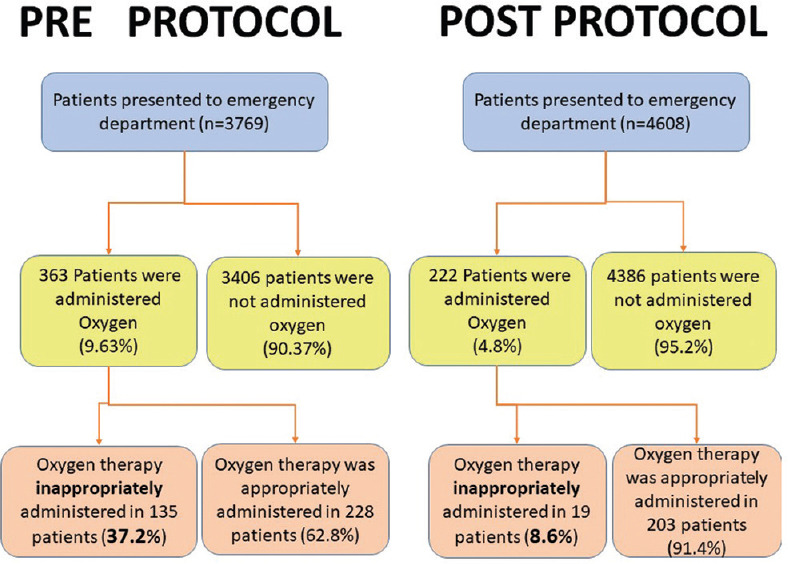
The 3-week pre-protocol observation phase in April 2016 included 3769 patients and the 3-week post-protocol observation phase in April 2017 included 4608 patients. The baseline demographic pattern was similar in both the pre-protocol and post-protocol groups. After the strict implementation of the algorithm, the number of patients receiving oxygen therapy decreased from 9.63% to 4.82%, a relative decrease of 51.4%. The average amount of total oxygen used decreased from 55.4 liters per person in pre-protocol group to 42.1 liters per person in the post-protocol group with a mean difference of 13.28 (95% CI 5.30-21.26; P = 0.001). Inappropriate oxygen usage decreased from 37.2% to 8.6%. There was a significant decrease in inappropriate oxygen use for indications like low sensorium (60.8% vs 21.7%) and trauma (88.5% vs 15.8%). The mortality rate in the pre-protocol phase was 2.7% as compared with 3.2% in the post-protocol phase. The total duration of inappropriate oxygen usage significantly decreased from 987 h to 89 h over the 21-day study period.
The implementation of an oxygen therapy algorithm significantly reduces inappropriate oxygen use and decreases treatment cost to the patient with no additional mortality risk.
尽管氧气是最古老的可用药物之一,但它仍然是使用最不当的药物之一,导致这种非常昂贵的资源被过度利用。
这项前瞻性观察性研究在印度一家大型急诊科进行。在严格实施氧气治疗算法前后,对氧气使用模式进行了研究。该算法传授给了所有医生和护士,并定期监测其实施情况。主要观察指标包括接受氧疗的患者比例、不当使用情况以及患者可避免的直接医疗费用。
2016年4月为期3周的方案前观察阶段纳入了3769例患者,2017年4月为期3周的方案后观察阶段纳入了4608例患者。方案前组和方案后组的基线人口统计学模式相似。严格实施算法后,接受氧疗的患者数量从9.63%降至4.82%,相对降幅为51.4%。总用氧量平均从方案前组的每人55.4升降至方案后组的每人42.1升,平均差异为13.28(95%可信区间5.30 - 21.26;P = 0.001)。不当氧疗使用情况从37.2%降至8.6%。对于诸如意识不清(60.8%对21.7%)和创伤(88.5%对15.8%)等指征,不当氧疗使用情况显著下降。方案前阶段的死亡率为2.7%,而方案后阶段为3.2%。在21天的研究期间,不当氧疗使用的总时长从987小时显著降至89小时。
实施氧气治疗算法可显著减少不当氧疗使用,并降低患者的治疗费用,且无额外的死亡风险。