Farber Nicholas J, Vij Sarah C, Shoskes Daniel A
Department of Urology, Glickman Urologic and Kidney Institute, Cleveland Clinic Foundation, Cleveland, OH, USA.
Transl Androl Urol. 2020 Jun;9(3):1108-1112. doi: 10.21037/tau-19-848.
The symptoms of hypogonadism are non-specific and restoring testosterone (T) to physiologic levels may not lead to clinical improvement. In men with a high burden of systemic illness, it is difficult to assess whether hypogonadism is a primary contributing factor of their symptoms. Given that testosterone replacement therapy (TRT) is not without risk, it is important to understand which patients will benefit from treatment. Therefore, we hypothesize that men with a higher burden of systemic illness would be less likely to continue with TRT.
We performed a retrospective review of our men's health registry for men who started TRT and adhered to follow up labs and visits within the first year. We restricted treatment to Testopel pellets due to reliable early T levels. Men were classified as yes/no for continued TRT based on whether they felt their presenting symptoms improved on therapy and they chose to continue TRT. The previously validated ACTIONS men's health phenotype was calculated as a composite systemic disease score grading severity [0-2] for each of anxiety, cardiovascular disease, low testosterone, diabetes, obesity, neurologic disease and obstructive sleep apnea (total score 0-14).
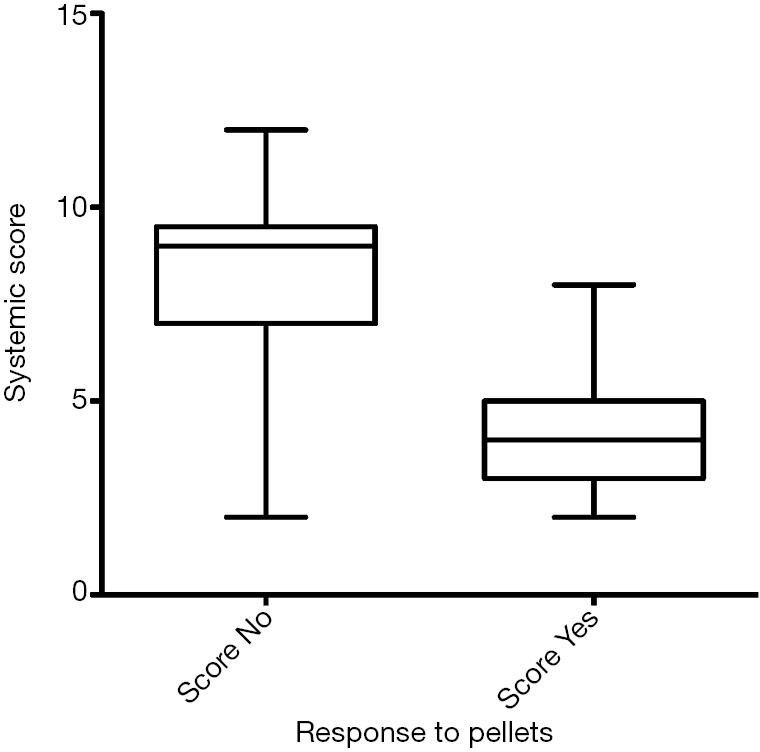
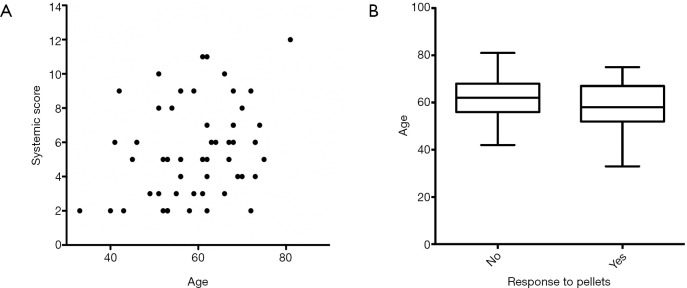
Sixty men were identified with a mean age of 59.5 (range, 33-81) years and mean starting total testosterone of 215 [48-332] ng/dL. Thirty-nine men (65%) felt symptomatic benefit and continued therapy for a median of 40.4 (20.5-76.4) months 21 men without benefit treated for a median of 4.1 months (2.9-10.7, P<0.0001). Those who stopped TRT had a higher ACTIONS score than those who continued (8±2.5 4.1±1.6, P<0.0001). Age weakly correlated with total ACTIONS score (r=0.28, P=0.03) but age had no impact on continuing TRT and the relationship between continuing TRT and ACTIONS score held true regardless of age.
Patients with a greater burden of systemic disease were less likely to have symptomatic improvement with TRT and more likely to stop therapy within a year. As several hypogonadal symptoms are non-specific, it is imperative that patients be counseled on the likelihood of success with TRT, particularly if they have multiple comorbidities. Ideal outcomes may come from multimodal therapy that includes lifestyle modification, and optimization of conditions such as diabetes, cardiovascular disease and sleep apnea.
性腺功能减退的症状不具有特异性,将睾酮(T)恢复到生理水平可能不会带来临床改善。在患有全身性疾病负担较重的男性中,很难评估性腺功能减退是否是其症状的主要促成因素。鉴于睾酮替代疗法(TRT)并非毫无风险,了解哪些患者将从治疗中获益很重要。因此,我们假设全身性疾病负担较重的男性继续接受TRT的可能性较小。
我们对男性健康登记处中开始接受TRT并在第一年内坚持进行随访实验室检查和就诊的男性进行了回顾性研究。由于早期T水平可靠,我们将治疗限制为Testopel颗粒。根据男性是否感觉其当前症状在治疗中有所改善以及他们是否选择继续接受TRT,将其分类为继续接受TRT/不继续接受TRT。先前经过验证的ACTIONS男性健康表型被计算为焦虑、心血管疾病、低睾酮、糖尿病、肥胖、神经系统疾病和阻塞性睡眠呼吸暂停每种疾病严重程度[0 - 2]的综合全身疾病评分(总分0 - 14)。
确定了60名男性,平均年龄为59.5(范围33 - 81)岁,平均起始总睾酮水平为215[48 - 332]ng/dL。39名男性(65%)感觉有症状改善并继续治疗,中位时间为40.4(20.5 - 76.4)个月;21名无改善的男性接受治疗的中位时间为4.1个月(2.9 - 10.7,P<0.0001)。停止TRT的患者的ACTIONS评分高于继续接受TRT的患者(8±2.5对4.1±1.6,P<0.0001)。年龄与总ACTIONS评分呈弱相关性(r = 0.28,P = 0.03),但年龄对继续接受TRT没有影响,并且无论年龄如何,继续接受TRT与ACTIONS评分之间的关系都成立。
全身性疾病负担较重的患者通过TRT获得症状改善的可能性较小,且更有可能在一年内停止治疗。由于几种性腺功能减退症状不具有特异性,必须向患者咨询TRT成功的可能性,特别是如果他们有多种合并症。理想的结果可能来自包括生活方式改变以及优化糖尿病、心血管疾病和睡眠呼吸暂停等病症的多模式治疗。